Bunions Causes Symptoms And Treatments
Overview
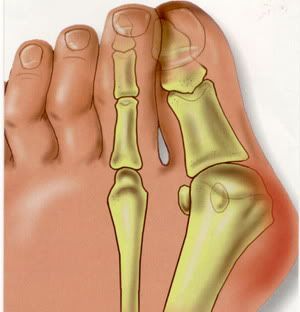 Bunions are one of the most common forefoot deformities. A displacement of the bone under the 1st toe occurs. This causes the big toe to move towards the smaller toes. This shifting of the bones causes a bony prominence on the side of the patients foot (the bunion joint). Over a period of time the big toe may come to rest under (occasionally over) the 2nd toe.
Bunions are one of the most common forefoot deformities. A displacement of the bone under the 1st toe occurs. This causes the big toe to move towards the smaller toes. This shifting of the bones causes a bony prominence on the side of the patients foot (the bunion joint). Over a period of time the big toe may come to rest under (occasionally over) the 2nd toe.
Causes
There are many factors which can contribute to the development of a bunion. The common causes are genetic factors, poor foot mechanics, high-heeled or narrow footwear and trauma to the toe. It is believed that constant stress on the joint of the big toe causes mild displacement of the bones and the joint, along with thickening of the tissues and a change in the pull of the muscles. This can result in a degree of arthritis of the joint, and over time, further displacement of the toe. This may lead to pain, difficultly with fitting shoes and corns/calloused lesions due to excess pressure on the smaller digits.
Symptoms
Audible clicking (called ?crepitus?) and/or stiffness in the affected joint which indicates that the joint surfaces are rubbing together improperly. Inflammation, degeneration of the surfaces of the joint, deformity (including bone growth at the joint line and displacement of the toe) and ultimately, loss of range of motion in the joint. Pain at the side and top of the joint that worsens with walking and physical activity.
Diagnosis
Diagnosis begins with a careful history and physical examination by your doctor. This will usually include a discussion about shoe wear and the importance of shoes in the development and treatment of the condition. X-rays will probably be suggested. This allows your doctor to measure several important angles made by the bones of the feet to help determine the appropriate treatment.
Non Surgical Treatment
A bunion may only need to be treated if it's severe and causing significant pain and discomfort. The different treatments for bunions are described below. If possible, non-surgical treatment for bunions will be used, which your GP can discuss with you. Non-surgical treatments can ease the pain and discomfort caused by a bunion, but they can't change the shape of your foot or prevent a bunion from getting worse over time. Non-surgical treatments include painkillers, bunion pads, orthotics, wearing suitable footwear, These are discussed in more detail below. If your bunion is painful, over-the-counter painkillers such as paracetamol or ibuprofen may be recommended.Bunion pads may also ease the pain of a bunion. Reusable bunion pads, made of either gel or fleece, are available over the counter from pharmacies. Some are adhesive and stick over the bunion, while others are held against your foot by a small loop that fits over your big toe. Bunion pads stop your foot rubbing on your shoe and relieve the pressure over the enlarged joint at the base of your big toe. Orthotics are placed inside your shoes to help realign the bones of your foot. They may help relieve the pressure on your bunion, which can ease the pain. However, there's little evidence that orthotics are effective in the long term. It's important that the orthotic fits properly, so you may want to seek advice from your GP or podiatrist (a specialist in diagnosing and treating foot conditions), who can suggest the best ones for you. 
Surgical Treatment
Surgery takes place either under local or general anaesthetic and takes about one hour. After surgery you will have either a plaster cast or special dressing on the foot and you will be given a special walking shoe and crutches to use the first few days/weeks. Recovery usually takes approximately 6-8 weeks but swelling often lasts longer and it may take a few months before you are able to wear normal shoes again. Full recovery can take up to a year. Bunion surgery is successful in approximately 85% of cases, but it is vital not to go back to wearing ill-fitting shoes else the problem is likely to return.
The Causes And Treatment Of Over-Pronation
Overview
Over-pronation is very common and affects millions of people. To better understand this condition, we'll take a closer look at the 3 most common foot types. An estimated 70% of the population has fallen arches (or a low arch). Only 20% has a normal arch. And 10% have abnormal feet, in other words they either have flat feet or the opposite a high arched foot.
Causes
Overpronation often occurs in people with flat feet, whose plantar fascia ligament is too flexible or too long, and therefore unable to properly support the longitudinal arch of the foot. People tend to inherit the foot structure that leads to overpronation. In a normal foot the bones are arranged so that two arches are formed, the longitudinal and the transverse. Ligaments hold all the bones in their correct positions, and tendons attach muscles to bones. If the bones are held together too loosely, they will tend to move inwards as this is the easiest direction for them to go. Over time the soft tissue structures will adjust to the misalignment and the foot will become permanently over-flexible, with a flat arch.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
Pronounced wear on the instep side of shoe heels can indicate overpronation, however it's best to get an accurate assessment. Footbalance retailers offer a free foot analysis to check for overpronation and help you learn more about your feet.
Non Surgical Treatment
Overpronation is usually corrected with orthotics and/or strengthening exercises for the tibialis posterior. Massage treatment can relieve myofascial trigger points in the tibialis posterior, and other muscles, and address any resulting neuromuscular dysfunction in the leg or foot. Biomechanical correction of overpronation might require orthotics, neuromuscular reeducation, or gait retraining methods, as well. Stretching the gastrocnemius and soleus muscles will reduce hypertonicity in these muscles and also is essential for effective treatment. Because of impacts throughout the remainder of the body, the detrimental effects of overpronation should not be overlooked.
Prevention
Pronation forces us to bear most of our weight on the inner border of our feet. Custom-made orthotics gently redistributes the weight so that the entire foot bears its normal share of weight with each step we take. The foot will not twist out at the ankle, but will strike the ground normally when the orthotics is used. This action of the custom-made orthotics will help to prevent shin splints, ankle sprains, knee and hip pain, lower back pain, nerve entrapments, tendonitis, muscle aches, bunions, generalized fatigue, hammer toes, and calluses.
Over-pronation is very common and affects millions of people. To better understand this condition, we'll take a closer look at the 3 most common foot types. An estimated 70% of the population has fallen arches (or a low arch). Only 20% has a normal arch. And 10% have abnormal feet, in other words they either have flat feet or the opposite a high arched foot.
Causes
Overpronation often occurs in people with flat feet, whose plantar fascia ligament is too flexible or too long, and therefore unable to properly support the longitudinal arch of the foot. People tend to inherit the foot structure that leads to overpronation. In a normal foot the bones are arranged so that two arches are formed, the longitudinal and the transverse. Ligaments hold all the bones in their correct positions, and tendons attach muscles to bones. If the bones are held together too loosely, they will tend to move inwards as this is the easiest direction for them to go. Over time the soft tissue structures will adjust to the misalignment and the foot will become permanently over-flexible, with a flat arch.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
Pronounced wear on the instep side of shoe heels can indicate overpronation, however it's best to get an accurate assessment. Footbalance retailers offer a free foot analysis to check for overpronation and help you learn more about your feet.
Non Surgical Treatment
Overpronation is usually corrected with orthotics and/or strengthening exercises for the tibialis posterior. Massage treatment can relieve myofascial trigger points in the tibialis posterior, and other muscles, and address any resulting neuromuscular dysfunction in the leg or foot. Biomechanical correction of overpronation might require orthotics, neuromuscular reeducation, or gait retraining methods, as well. Stretching the gastrocnemius and soleus muscles will reduce hypertonicity in these muscles and also is essential for effective treatment. Because of impacts throughout the remainder of the body, the detrimental effects of overpronation should not be overlooked.
Prevention
Pronation forces us to bear most of our weight on the inner border of our feet. Custom-made orthotics gently redistributes the weight so that the entire foot bears its normal share of weight with each step we take. The foot will not twist out at the ankle, but will strike the ground normally when the orthotics is used. This action of the custom-made orthotics will help to prevent shin splints, ankle sprains, knee and hip pain, lower back pain, nerve entrapments, tendonitis, muscle aches, bunions, generalized fatigue, hammer toes, and calluses.
Does Calcaneal Apophysitis Necessitate Surgical Procedures?
Overview
Sever disease, first described in 1912, is a painful inflammation of the calcaneal apophysis. It is classified with the child and adolescent nonarticular osteochondroses. (The other disease in this group is Iselin disease, which is inflammation of the base of the fifth metatarsal.) The etiology of pain in Sever disease is believed to be repetitive trauma to the weaker structure of the apophysis, induced by the pull of the tendo calcaneus (Achilles tendon) on its insertion. This results in a clinical picture of heel pain in a growing active child, which worsens with activity. Sever disease is a self-limited condition; accordingly, no known complication exists from failure to make the correct diagnosis.
Causes
This condition is more common in boys than girls. It generally presents between the ages of 9-14 and peaks between ages 10-12 years. This injury can reoccur up until the age of 17, when the growth plate of the calcaneous generally closes. These types of injuries will commonly occur during periods of rapid growth. Sever?s Disease occurs more frequently in child with flat feet, but all children with flat feet will not get Sever?s.
Symptoms
Pain symptoms usually begin after a child begins a new sport or sporting season, and can worsen with athletic activities that involve running and jumping. It is common for a child with Sever?s disease to walk with a limp. Increased activity can lead to heel cord tightness (Achilles Tendon), resulting in pressure on the apophysis of the calcaneus. This will cause irritation of the growth plate and sometimes swelling in the heel area thus producing pain. This usually occurs in the early stages of puberty.
Diagnosis
A physical exam of the heel will show tenderness over the back of the heel but not in the Achilles tendon or plantar fascia. There may be tightness in the calf muscle, which contributes to tension on the heel. The tendons in the heel get stretched more in patients with flat feet. There is greater impact force on the heels of athletes with a high-arched, rigid foot. The doctor may order an x-ray because x-rays can confirm how mature the growth center is and if there are other sources of heel pain, such as a stress fracture or bone cyst. However, x-rays are not necessary to diagnose Sever?s disease, and it is not possible to make the diagnosis based on the x-ray alone.
Non Surgical Treatment
The aim of treatment is to reduce the pain and inflammation when gently stretch the muscles. There is likely to be no magic instant cure and the young athlete may have to be patient while they grow. Rest and apply ice or cold therapy to the heel. Do not apply ice directly to the skin but wrap in a wet tea towel to avoid ice burns. Rest from activities which cause pain. If running and playing football makes it worse then reduce or stop this activity and try cycling or swimming to maintain fitness. A temporary measure is to insert a heel pad or heel raise into the shoes. This has the effect of raising the heel and shortening the calf muscles and so taking the strain off the back of the heel. However long term use of a heal raise may shorten the calf muscles when they need stretching. Stretch the calf muscles regularly. Stretching should be done pain free and very gently with this injury. See a sports injury professional who can advise on treatment and rehabilitation.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position. If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
Sever disease, first described in 1912, is a painful inflammation of the calcaneal apophysis. It is classified with the child and adolescent nonarticular osteochondroses. (The other disease in this group is Iselin disease, which is inflammation of the base of the fifth metatarsal.) The etiology of pain in Sever disease is believed to be repetitive trauma to the weaker structure of the apophysis, induced by the pull of the tendo calcaneus (Achilles tendon) on its insertion. This results in a clinical picture of heel pain in a growing active child, which worsens with activity. Sever disease is a self-limited condition; accordingly, no known complication exists from failure to make the correct diagnosis.
Causes
This condition is more common in boys than girls. It generally presents between the ages of 9-14 and peaks between ages 10-12 years. This injury can reoccur up until the age of 17, when the growth plate of the calcaneous generally closes. These types of injuries will commonly occur during periods of rapid growth. Sever?s Disease occurs more frequently in child with flat feet, but all children with flat feet will not get Sever?s.
Symptoms
Pain symptoms usually begin after a child begins a new sport or sporting season, and can worsen with athletic activities that involve running and jumping. It is common for a child with Sever?s disease to walk with a limp. Increased activity can lead to heel cord tightness (Achilles Tendon), resulting in pressure on the apophysis of the calcaneus. This will cause irritation of the growth plate and sometimes swelling in the heel area thus producing pain. This usually occurs in the early stages of puberty.
Diagnosis
A physical exam of the heel will show tenderness over the back of the heel but not in the Achilles tendon or plantar fascia. There may be tightness in the calf muscle, which contributes to tension on the heel. The tendons in the heel get stretched more in patients with flat feet. There is greater impact force on the heels of athletes with a high-arched, rigid foot. The doctor may order an x-ray because x-rays can confirm how mature the growth center is and if there are other sources of heel pain, such as a stress fracture or bone cyst. However, x-rays are not necessary to diagnose Sever?s disease, and it is not possible to make the diagnosis based on the x-ray alone.
Non Surgical Treatment
The aim of treatment is to reduce the pain and inflammation when gently stretch the muscles. There is likely to be no magic instant cure and the young athlete may have to be patient while they grow. Rest and apply ice or cold therapy to the heel. Do not apply ice directly to the skin but wrap in a wet tea towel to avoid ice burns. Rest from activities which cause pain. If running and playing football makes it worse then reduce or stop this activity and try cycling or swimming to maintain fitness. A temporary measure is to insert a heel pad or heel raise into the shoes. This has the effect of raising the heel and shortening the calf muscles and so taking the strain off the back of the heel. However long term use of a heal raise may shorten the calf muscles when they need stretching. Stretch the calf muscles regularly. Stretching should be done pain free and very gently with this injury. See a sports injury professional who can advise on treatment and rehabilitation.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position. If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
Causes Of Acquired Flat Foot
Overview
Many foot problems can be contributed to Adult Acquired Flatfoot Deformity (AAFD), a foot and ankle condition that causes fallen arch of the foot. AAFD is also referred to as Posterior Tibial Tendon Dysfunction (PTTD). The posterior tibial tendon serves as the principal supporting structure of your foot. When this ligament is injured overtime the arches start to flatten, leaving you with a painful foot condition. AAFD is more common in women ages 39 - 65 than men. 
Causes
The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction. What causes adult acquired flat foot? Fracture or dislocation. Tendon laceration. Tarsal Coalition. Arthritis. Neuroarthropathy. Neurological weakness.
Symptoms
Patients often experience pain and/or deformity at the ankle or hindfoot. When the posterior tibial tendon does not work properly, a number of changes can occur to the foot and ankle. In the earlier stages, symptoms often include pain and tenderness along the posterior tibial tendon behind the inside of the ankle. As the tendon progressively fails, deformity of the foot and ankle may occur. This deformity can include progressive flattening of the arch, shifting of the heel so that it no longer is aligned underneath the rest of the leg, rotation and deformity of the forefoot, tightening of the heel cord, development of arthritis, and deformity of the ankle joint. At certain stages of this disorder, pain may shift from the inside to the outside aspect of the ankle as the heel shifts outward and structures are pinched laterally.
Diagnosis
The history and physical examination are probably the most important tools the physician uses to diagnose this problem. The wear pattern on your shoes can offer some helpful clues. Muscle testing helps identify any areas of weakness or muscle impairment. This should be done in both the weight bearing and nonweight bearing positions. A very effective test is the single heel raise. You will be asked to stand on one foot and rise up on your toes. You should be able to lift your heel off the ground easily while keeping the calcaneus (heel bone) in the middle with slight inversion (turned inward). X-rays are often used to study the position, shape, and alignment of the bones in the feet and ankles. Magnetic resonance (MR) imaging is the imaging modality of choice for evaluating the posterior tibial tendon and spring ligament complex.
Non surgical Treatment
A patient who has acute tenosynovitis has pain and swelling along the medial aspect of the ankle. The patient is able to perform a single-limb heel-rise test but has pain when doing so. Inversion of the foot against resistance is painful but still strong. The patient should be managed with rest, the administration of appropriate anti-inflammatory medication, and immobilization. The injection of corticosteroids is not recommended. Immobilization with either a rigid below-the-knee cast or a removable cast or boot may be used to prevent overuse and subsequent rupture of the tendon. A removable stirrup-brace is not initially sufficient as it does not limit motion in the sagittal plane, a component of the pathological process. The patient should be permitted to walk while wearing the cast or boot during the six to eight-week period of immobilization. At the end of that time, a decision must be made regarding the need for additional treatment. If there has been marked improvement, the patient may begin wearing a stiff-soled shoe with a medial heel-and-sole wedge to invert the hindfoot. If there has been only mild or moderate improvement, a longer period in the cast or boot may be tried. 
Surgical Treatment
The indications for surgery are persistent pain and/or significant deformity. Sometimes the foot just feels weak and the assessment of deformity is best done by a foot and ankle specialist. If surgery is appropriate, a combination of soft tissue and bony procedures may be considered to correct alignment and support the medial arch, taking strain off failing ligaments. Depending upon the tissues involved and extent of deformity, the foot and ankle specialist will determine the necessary combination of procedures. Surgical procedures may include a medial slide calcaneal osteotomy to correct position of the heel, a lateral column lengthening to correct position in the midfoot and a medial cuneiform osteotomy or first metatarsal-tarsal fusion to correct elevation of the medial forefoot. The posterior tibial tendon may be reconstructed with a tendon transfer. In severe cases (stage III), the reconstruction may include fusion of the hind foot,, resulting in stiffness of the hind foot but the desired pain relief. In the most severe stage (stage IV), the deltoid ligament on the inside of the ankle fails, resulting in the deformity in the ankle. This deformity over time can result in arthritis in the ankle.
Adult Aquired FlatFoot Reality
Overview
There are four stages of posterior tibial tendon dysfunction. In the first stage the posterior tibial tendon is inflamed but has normal strength. There is little to no change in the arch of the foot. In stage two the tendon is partially torn or shows degenerative changes and as a result loses strength. There is considerable flattening of the arch without arthritic changes in the foot. Stage three results when the posterior tibial tendon is torn and not functioning. As a result the arch is completely collapsed with arthritic changes in the foot. Stage four is identical to stage three except that the ankle joint also becomes arthritic.
Causes
There are numerous causes of acquired Adult Flatfoot, including, trauma, fracture, dislocation, tendon rupture/partial rupture or inflammation of the tendons, tarsal coalition, arthritis, neuroarthropathy and neurologic weakness. The most common cause of acquired Adult Flatfoot is due to overuse of a tendon on the inside of the ankle called the posterior tibial tendon. This is classed as - posterior tibial tendon dysfunction. What are the causes of Adult Acquired flat foot? Trauma, Fracture or dislocation. Tendon rupture, partial tear or inflammation. Tarsal Coalition. Arthritis. Neuroarthropathy. Neurological weakness.
Symptoms
Pain and swelling behind the inside of your ankle and along your instep. You may be tender behind the inner ankle where the posterior tibial tendon courses and occasionally get burning, shooting, tingling or stabbing pain as a result of inflammation of the nerve inside the tarsal tunnel. Difficulty walking, the inability to walk long distances and a generalised ache while walking even short distances. This may probably become more pronounced at the end of each day. Change in foot shape, sometimes your tendon stretches out, this is due to weakening of the tendon and ligaments. When this occurs, the arch in your foot flattens and a flatfoot deformity occurs, presenting a change in foot shape. Inability to tip-toe, a way of diagnosing Posterior Tibial Tendon Dysfunction is difficulty or inability to ?heel rise? (stand on your toes on one foot). Your tibialis posterior tendon enables you to perform this manoeuvre effectively. You may also experience pain upon attempting to perform a heel rise.
Diagnosis
The adult acquired flatfoot, secondary to posterior tibial tendon dysfunction, is diagnosed in a number of ways with no single test proven to be totally reliable. The most accurate diagnosis is made by a skilled clinician utilizing observation and hands on evaluation of the foot and ankle. Observation of the foot in a walking examination is most reliable. The affected foot appears more pronated and deformed compared to the unaffected foot. Muscle testing will show a strength deficit. An easy test to perform in the office is the single foot raise. A patient is asked to step with full body weight on the symptomatic foot, keeping the unaffected foot off the ground. The patient is then instructed to "raise up on the tip toes" of the affected foot. If the posterior tibial tendon has been attenuated or ruptured, the patient will be unable to lift the heel off the floor and rise onto the toes. In less severe cases, the patient will be able to rise on the toes, but the heel will not be noted to invert as it normally does when we rise onto the toes. X-rays can be helpful but are not diagnostic of the adult acquired flatfoot. Both feet - the symptomatic and asymptomatic - will demonstrate a flatfoot deformity on x-ray. Careful observation may show a greater severity of deformity on the affected side.
Non surgical Treatment
Conservative (nonoperative) care is advised at first. A simple modification to your shoe may be all that???s needed. Sometimes purchasing shoes with a good arch support is sufficient. For other patients, an off-the-shelf (prefabricated) shoe insert works well. The orthotic is designed specifically to position your foot in good alignment. Like the shoe insert, the orthotic fits inside the shoe. These work well for mild deformity or symptoms. Over-the-counter pain relievers or antiinflammatory drugs such as ibuprofen may be helpful. If symptoms are very severe, a removable boot or cast may be used to rest, support, and stabilize the foot and ankle while still allowing function. Patients with longer duration of symptoms or greater deformity may need a customized brace. The brace provides support and limits ankle motion. After several months, the brace is replaced with a foot orthotic. A physical therapy program of exercise to stretch and strengthen the foot and leg muscles is important. The therapist will also show you how to improve motor control and proprioception (joint sense of position). These added features help prevent and reduce injuries.

Surgical Treatment
When conservative care fails to control symptoms and/or deformity, then surgery may be needed. The goal of surgical treatment is to obtain good alignment while keeping the foot and ankle as flexible as possible. The most common procedures used with this condition include arthrodesis (fusion), osteotomy (cutting out a wedge-shaped piece of bone), and lateral column lengthening. Lateral column lengthening involves the use of a bone graft at the calcaneocuboid joint. This procedure helps restore the medial longitudinal arch (arch along the inside of the foot). A torn tendon or spring ligament will be repaired or reconstructed. Other surgical options include tendon shortening or lengthening. Or the surgeon may move one or more tendons. This procedure is called a tendon transfer. Tendon transfer uses another tendon to help the posterior tibial tendon function more effectively. A tendon transfer is designed to change the force and angle of pull on the bones of the arch. It's not clear yet from research evidence which surgical procedure works best for this condition. A combination of surgical treatments may be needed. It may depend on your age, type and severity of deformity and symptoms, and your desired level of daily activity.
There are four stages of posterior tibial tendon dysfunction. In the first stage the posterior tibial tendon is inflamed but has normal strength. There is little to no change in the arch of the foot. In stage two the tendon is partially torn or shows degenerative changes and as a result loses strength. There is considerable flattening of the arch without arthritic changes in the foot. Stage three results when the posterior tibial tendon is torn and not functioning. As a result the arch is completely collapsed with arthritic changes in the foot. Stage four is identical to stage three except that the ankle joint also becomes arthritic.
Causes
There are numerous causes of acquired Adult Flatfoot, including, trauma, fracture, dislocation, tendon rupture/partial rupture or inflammation of the tendons, tarsal coalition, arthritis, neuroarthropathy and neurologic weakness. The most common cause of acquired Adult Flatfoot is due to overuse of a tendon on the inside of the ankle called the posterior tibial tendon. This is classed as - posterior tibial tendon dysfunction. What are the causes of Adult Acquired flat foot? Trauma, Fracture or dislocation. Tendon rupture, partial tear or inflammation. Tarsal Coalition. Arthritis. Neuroarthropathy. Neurological weakness.
Symptoms
Pain and swelling behind the inside of your ankle and along your instep. You may be tender behind the inner ankle where the posterior tibial tendon courses and occasionally get burning, shooting, tingling or stabbing pain as a result of inflammation of the nerve inside the tarsal tunnel. Difficulty walking, the inability to walk long distances and a generalised ache while walking even short distances. This may probably become more pronounced at the end of each day. Change in foot shape, sometimes your tendon stretches out, this is due to weakening of the tendon and ligaments. When this occurs, the arch in your foot flattens and a flatfoot deformity occurs, presenting a change in foot shape. Inability to tip-toe, a way of diagnosing Posterior Tibial Tendon Dysfunction is difficulty or inability to ?heel rise? (stand on your toes on one foot). Your tibialis posterior tendon enables you to perform this manoeuvre effectively. You may also experience pain upon attempting to perform a heel rise.
Diagnosis
The adult acquired flatfoot, secondary to posterior tibial tendon dysfunction, is diagnosed in a number of ways with no single test proven to be totally reliable. The most accurate diagnosis is made by a skilled clinician utilizing observation and hands on evaluation of the foot and ankle. Observation of the foot in a walking examination is most reliable. The affected foot appears more pronated and deformed compared to the unaffected foot. Muscle testing will show a strength deficit. An easy test to perform in the office is the single foot raise. A patient is asked to step with full body weight on the symptomatic foot, keeping the unaffected foot off the ground. The patient is then instructed to "raise up on the tip toes" of the affected foot. If the posterior tibial tendon has been attenuated or ruptured, the patient will be unable to lift the heel off the floor and rise onto the toes. In less severe cases, the patient will be able to rise on the toes, but the heel will not be noted to invert as it normally does when we rise onto the toes. X-rays can be helpful but are not diagnostic of the adult acquired flatfoot. Both feet - the symptomatic and asymptomatic - will demonstrate a flatfoot deformity on x-ray. Careful observation may show a greater severity of deformity on the affected side.
Non surgical Treatment
Conservative (nonoperative) care is advised at first. A simple modification to your shoe may be all that???s needed. Sometimes purchasing shoes with a good arch support is sufficient. For other patients, an off-the-shelf (prefabricated) shoe insert works well. The orthotic is designed specifically to position your foot in good alignment. Like the shoe insert, the orthotic fits inside the shoe. These work well for mild deformity or symptoms. Over-the-counter pain relievers or antiinflammatory drugs such as ibuprofen may be helpful. If symptoms are very severe, a removable boot or cast may be used to rest, support, and stabilize the foot and ankle while still allowing function. Patients with longer duration of symptoms or greater deformity may need a customized brace. The brace provides support and limits ankle motion. After several months, the brace is replaced with a foot orthotic. A physical therapy program of exercise to stretch and strengthen the foot and leg muscles is important. The therapist will also show you how to improve motor control and proprioception (joint sense of position). These added features help prevent and reduce injuries.
Surgical Treatment
When conservative care fails to control symptoms and/or deformity, then surgery may be needed. The goal of surgical treatment is to obtain good alignment while keeping the foot and ankle as flexible as possible. The most common procedures used with this condition include arthrodesis (fusion), osteotomy (cutting out a wedge-shaped piece of bone), and lateral column lengthening. Lateral column lengthening involves the use of a bone graft at the calcaneocuboid joint. This procedure helps restore the medial longitudinal arch (arch along the inside of the foot). A torn tendon or spring ligament will be repaired or reconstructed. Other surgical options include tendon shortening or lengthening. Or the surgeon may move one or more tendons. This procedure is called a tendon transfer. Tendon transfer uses another tendon to help the posterior tibial tendon function more effectively. A tendon transfer is designed to change the force and angle of pull on the bones of the arch. It's not clear yet from research evidence which surgical procedure works best for this condition. A combination of surgical treatments may be needed. It may depend on your age, type and severity of deformity and symptoms, and your desired level of daily activity.
What Are The Primary Causes And Treatments Of Achilles Tendonitis Discomfort ?
Overview
 Achilles tendinitis is an irritation/inflammation in the achilles tendon, which attaches to the back of the heel. It is often a result of overuse and occurs frequently in runners who have altered their training suddenly, either with regard to duration or intensity. This injury is also prevalent in middle-aged people who are active.
Achilles tendinitis is an irritation/inflammation in the achilles tendon, which attaches to the back of the heel. It is often a result of overuse and occurs frequently in runners who have altered their training suddenly, either with regard to duration or intensity. This injury is also prevalent in middle-aged people who are active.
Causes
Like any muscle or tendon in the body, the older we get, the more likely we are to sustain an injury. So middle-aged men and women are most at risk, with a slightly higher risk factor attributed to males. Those who participate in more intense athletic activities like high impact sports (tennis, running, basketball) are most susceptible to the injury. Certain underlying medical conditions can also be a contributing factor. Diabetics are more at risk of suffering from Achilles Tendinitis, as are those who are not in great physical shape. Some antibiotics, particularly fluoroquinolones can make one more likely to suffer a strained Achilles Tendon.
Symptoms
There will be a gradual onset of achilles tendon pain over a period of weeks, or even months. The pain will come on during exercise and is constant throughout the training session. Pain will be felt in the achilles tendon when walking especially up hill or up stairs. This is because the achilles is having to stretch further than normal. There is likely to be stiffness in the Achilles tendon especially in the morning or after a long period of rest. This is thought to be due to adhesions between the tendon sheath and the tendon itself. Nodules or lumps may be found in the achilles tendon, particularly 2-4cm above the heel and the skin will appear red. Pain and tenderness will be felt when pressing in on the achilles tendon which is likely to appear thickened or swollen. A creaking sensation may be felt when press the fingers into the sides of the tendon and moving the ankle.This is known as crepitus.
Diagnosis
During the physical exam, your doctor will gently press on the affected area to determine the location of pain, tenderness or swelling. He or she will also evaluate the flexibility, alignment, range of motion and reflexes of your foot and ankle. Your doctor may order one or more of the following tests to assess your condition, X-rays. While X-rays can't visualize soft tissues such as tendons, they may help rule out other conditions that can cause similar symptoms. Ultrasound. This device uses sound waves to visualize soft tissues like tendons. Ultrasound can also produce real-time images of the Achilles tendon in motion. Magnetic resonance imaging (MRI). Using radio waves and a very strong magnet, MRI machines can produce very detailed images of the Achilles tendon.
Nonsurgical Treatment
If caught early enough, simple physical therapy that you can do by yourself should be fine. Over the counter solutions as easy as pain medication, cold compresses, a different pair of shoes, or a new set of stretching exercises can make most of the symptoms of Achilles tendinitis disappear. Further trouble or extreme pain should be regarded as a sign that something more serious is wrong, and you should immediately consult a doctor or physician. They will look to see whether non-surgical or surgical methods are your best options, and from there you can determine what your budget is for dealing with the condition.

Surgical Treatment
Not every Achilles tendon injury or condition requires surgery. It is generally understood by doctors and surgeons, that surgery will introduce more scar tissue into the Achilles tendon. This added scar tissue will be problematic, requiring physical therapy and conservative treatment options post-surgery. If not dealt with properly, your ankle and Achilles tendon could end up in worse condition than before the surgery! This is why surgery is only performed as a last resort.
Prevention
There are several things you can do to reduce the risk of Achilles tendinitis, warm up every time before you exercise or play a sport. Switch up your exercises. Slowly increase the length and intensity of your workouts. Keep your muscles active and stay in shape all year-round. When you see symptoms of Achilles tendinitis, stop whatever activity you are doing and rest.
Achilles tendinitis is an irritation/inflammation in the achilles tendon, which attaches to the back of the heel. It is often a result of overuse and occurs frequently in runners who have altered their training suddenly, either with regard to duration or intensity. This injury is also prevalent in middle-aged people who are active.
Causes
Like any muscle or tendon in the body, the older we get, the more likely we are to sustain an injury. So middle-aged men and women are most at risk, with a slightly higher risk factor attributed to males. Those who participate in more intense athletic activities like high impact sports (tennis, running, basketball) are most susceptible to the injury. Certain underlying medical conditions can also be a contributing factor. Diabetics are more at risk of suffering from Achilles Tendinitis, as are those who are not in great physical shape. Some antibiotics, particularly fluoroquinolones can make one more likely to suffer a strained Achilles Tendon.
Symptoms
There will be a gradual onset of achilles tendon pain over a period of weeks, or even months. The pain will come on during exercise and is constant throughout the training session. Pain will be felt in the achilles tendon when walking especially up hill or up stairs. This is because the achilles is having to stretch further than normal. There is likely to be stiffness in the Achilles tendon especially in the morning or after a long period of rest. This is thought to be due to adhesions between the tendon sheath and the tendon itself. Nodules or lumps may be found in the achilles tendon, particularly 2-4cm above the heel and the skin will appear red. Pain and tenderness will be felt when pressing in on the achilles tendon which is likely to appear thickened or swollen. A creaking sensation may be felt when press the fingers into the sides of the tendon and moving the ankle.This is known as crepitus.
Diagnosis
During the physical exam, your doctor will gently press on the affected area to determine the location of pain, tenderness or swelling. He or she will also evaluate the flexibility, alignment, range of motion and reflexes of your foot and ankle. Your doctor may order one or more of the following tests to assess your condition, X-rays. While X-rays can't visualize soft tissues such as tendons, they may help rule out other conditions that can cause similar symptoms. Ultrasound. This device uses sound waves to visualize soft tissues like tendons. Ultrasound can also produce real-time images of the Achilles tendon in motion. Magnetic resonance imaging (MRI). Using radio waves and a very strong magnet, MRI machines can produce very detailed images of the Achilles tendon.
Nonsurgical Treatment
If caught early enough, simple physical therapy that you can do by yourself should be fine. Over the counter solutions as easy as pain medication, cold compresses, a different pair of shoes, or a new set of stretching exercises can make most of the symptoms of Achilles tendinitis disappear. Further trouble or extreme pain should be regarded as a sign that something more serious is wrong, and you should immediately consult a doctor or physician. They will look to see whether non-surgical or surgical methods are your best options, and from there you can determine what your budget is for dealing with the condition.
Surgical Treatment
Not every Achilles tendon injury or condition requires surgery. It is generally understood by doctors and surgeons, that surgery will introduce more scar tissue into the Achilles tendon. This added scar tissue will be problematic, requiring physical therapy and conservative treatment options post-surgery. If not dealt with properly, your ankle and Achilles tendon could end up in worse condition than before the surgery! This is why surgery is only performed as a last resort.
Prevention
There are several things you can do to reduce the risk of Achilles tendinitis, warm up every time before you exercise or play a sport. Switch up your exercises. Slowly increase the length and intensity of your workouts. Keep your muscles active and stay in shape all year-round. When you see symptoms of Achilles tendinitis, stop whatever activity you are doing and rest.
What Is Plantar Fasciitis And Learn How To End It

Overview
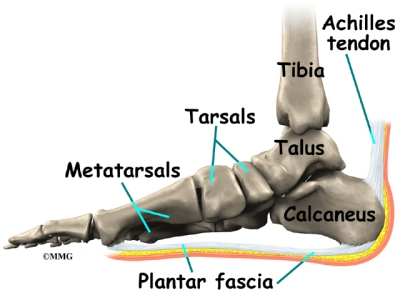
Plantar Fasciitis is an inflammation caused by excessive stretching of the plantar fascia. The plantar fascia is a broad band of fibrous tissue which runs along the bottom surface of the foot, attaching at the bottom of the heel bone and extending to the forefoot. When the plantar fascia is excessively stretched, this can cause plantar fasciitis, which can also lead to heel pain, arch pain, and heel spurs.
Causes
A variety of causes exist for plantar fasciitis. Some of the most common causes include excessive weight load on the foot due to obesity or prolonged standing, mechanical imbalances of the foot, osteoarthritis and rheumatoid arthritis, sudden increase in body weight (e.g., pregnancy), sudden increase in walking or running, tight calf muscles is a very common cause of the disorder, wearing shoes with poor support, including flip-flops. Another cause of pain is the shortening of the plantar fascia overnight due to the ankle bending, causing the toes to point towards the ground. The plantar fascia stretches in the morning when you stand. The act of lengthening it causes a great deal of pain. However, this is not limited to an overnight occurrence, it can happen any time the foot is flexed (i.e., pointed) for extended periods of time. For example, driving in the car for long periods can cause fasciitis in the right foot, which steps on the accelerator.
Symptoms
A sharp pain in the center of your heel will most likely be one of the biggest symptoms of plantar fasciitis. A classic sign of plantar fasciitis is when the pain is worst during the first steps you take in the morning.
Diagnosis
During the physical exam, your doctor checks for points of tenderness in your foot. The location of your pain can help determine its cause. Usually no tests are necessary. The diagnosis is made based on the history and physical examination. Occasionally your doctor may suggest an X-ray or magnetic resonance imaging (MRI) to make sure your pain isn't being caused by another problem, such as a stress fracture or a pinched nerve. Sometimes an X-ray shows a spur of bone projecting forward from the heel bone. In the past, these bone spurs were often blamed for heel pain and removed surgically. But many people who have bone spurs on their heels have no heel pain.
Non Surgical Treatment
Reducing inflammation in the plantar fascia ligament is an important part of treatment, though this does not address the underlying damage to the ligament. Initial home treatment includes staying off your feet and applying ice for 15 to 20 minutes three or four times a day to reduce swelling. You can also try reducing or changing your exercise activities. Using arch supports in your shoes and doing stretching exercises may also help to relieve pain. Nonsteroidal anti-inflammatory drugs (NSAIDS), such as ibuprofen (i.e. Motrin or Advil) and naproxen (i.e. Aleve), are often used to reduce inflammation in the ligament. If home treatments and over-the-counter anti-inflammatory drugs don’t ease the pain, an injection of a corticosteroid directly into the damaged section of the ligament can be given. Your doctor can do this in his or her office. Your doctor may use an ultrasound device to help determine the best place for the injection. Corticosteroids can also be administered on the skin of your heel or the arch of your foot, and then a painless electrical current is applied to let the steroid pass through your skin and into the muscle. Physical therapy is an important part of treatment for planter fasciitis. It can help stretch your plantar fascia and Achilles tendons. A physical therapist can also show you exercises to strengthen your lower leg muscles, helping to stabilize your walk and lessen the workload on your plantar fascia. If pain continues and other methods aren’t working, your doctor may recommend extracorporeal shock wave therapy. Sound waves are bombarded against your heel to stimulate healing within the ligament. This treatment can result in bruises, swelling, pain, and numbness, and has not been proven to be consistently effective in relieving symptoms.
Surgical Treatment
Surgery is considered only after 12 months of aggressive nonsurgical treatment. Gastrocnemius recession. This is a surgical lengthening of the calf (gastrocnemius) muscles. Because tight calf muscles place increased stress on the plantar fascia, this procedure is useful for patients who still have difficulty flexing their feet, despite a year of calf stretches. In gastrocnemius recession, one of the two muscles that make up the calf is lengthened to increase the motion of the ankle. The procedure can be performed with a traditional, open incision or with a smaller incision and an endoscope, an instrument that contains a small camera. Your doctor will discuss the procedure that best meets your needs. Complication rates for gastrocnemius recession are low, but can include nerve damage. Plantar fascia release. If you have a normal range of ankle motion and continued heel pain, your doctor may recommend a partial release procedure. During surgery, the plantar fascia ligament is partially cut to relieve tension in the tissue. If you have a large bone spur, it will be removed, as well. Although the surgery can be performed endoscopically, it is more difficult than with an open incision. In addition, endoscopy has a higher risk of nerve damage.
Stretching Exercises
Calf stretch. Lean forward against a wall with one knee straight and the heel on the ground. Place the other leg in front, with the knee bent. To stretch the calf muscles and the heel cord, push your hips toward the wall in a controlled fashion. Hold the position for 10 seconds and relax. Repeat this exercise 20 times for each foot. A strong pull in the calf should be felt during the stretch. Plantar fascia stretch. This stretch is performed in the seated position. Cross your affected foot over the knee of your other leg. Grasp the toes of your painful foot and slowly pull them toward you in a controlled fashion. If it is difficult to reach your foot, wrap a towel around your big toe to help pull your toes toward you. Place your other hand along the plantar fascia. The fascia should feel like a tight band along the bottom of your foot when stretched. Hold the stretch for 10 seconds. Repeat it 20 times for each foot. This exercise is best done in the morning before standing or walking.