Bursitis Of The Feet Bursa Removal Complications
Overview
Retrocalcaneal bursitis is an inflammation of the bursa at the back of the heel bone (calcaneus). This causes pain with up-and-down movements of the foot. Alternative name is Insertional heel pain.
Causes
Occasionally the bursal sac can become inflamed and painful. Pain to the region is worse typically with initial weight bearing activity such as rising from bed in the morning. Swelling and warmth to the region are common. Clinical examination shows pain to palpation at the retrocalcaneus at a level just before the Achilles tendon. Increase pressure and friction of the Achilles tendon across the retrocalcaneal region is the cause of this bursitis. A high arch, tight Achilles tendon or bone spur appear to be some of the main causes of this problem. With a high arch the back portion of the calcaneus abnormally projects into the Achilles tendon region.
Symptoms
Pain and tenderness are common symptoms. If the affected joint is close to the skin, as with the shoulder, knee, elbow, or Achilles tendon, swelling and redness are seen and the area may feel warm to the touch. The bursae around the hip joint are deeper, and swelling is not obvious. Movement may be limited and is painful. In the shoulder, it may be difficult to raise the arm out from the side of the body. Putting on a jacket or combing the hair becomes a troublesome activity. In acute bursitis symptoms appear suddenly, with chronic bursitis, pain, tenderness, and limited movement reappear after exercise or strain.
Diagnosis
Diagnosis is first by clinical suspicion of symptoms. This can be mistaken for gout or infection especially in the big toe region. A diagnosis of bursitis is usually used in combination of the underlying cause, for instance a bunion deformity, Haglund's deformity, or Heel Spur Syndrome. Many times the cause needs to be addressed to rid the problem of bursitis.
Non Surgical Treatment
Your health care provider may recommend the following treatments. Avoid activities that cause pain. Ice the heel several times a day. Take nonsteroidal anti-inflammatory medications (for example, ibuprofen). Try over-the-counter or custom heel wedges to help decrease the stress on the heel. Try ultrasound treatment during physical therapy to reduce inflammation. Use physical therapy to improve flexibility and strength around the ankle, which can help the bursitis improve and prevent it from coming back. If these treatments don't work, your health care provider may inject a small amount of steroids into the bursa. After the injection, you should avoid stretching the tendon too much because it can break open (rupture). If the condition is connected with Achilles tendinitis, casting the ankle for several weeks to keep it from moving can be effective. Very rarely, surgery may be needed to remove the inflamed bursa.
Prevention
Contact your physician if bursitis pain is disabling (when movement of the joint is largely or entirely restricted), if the pain doesn?t subside after a week of self-care, or if the joint is red and swollen. Also call your doctor if you develop a fever, which could signal infectious bursitis-a condition that especially can afflict the elbow. Except for the fever, symptoms resemble other forms of bursitis, but infectious bursitis requires immediate medical attention.
Retrocalcaneal bursitis is an inflammation of the bursa at the back of the heel bone (calcaneus). This causes pain with up-and-down movements of the foot. Alternative name is Insertional heel pain.
Causes
Occasionally the bursal sac can become inflamed and painful. Pain to the region is worse typically with initial weight bearing activity such as rising from bed in the morning. Swelling and warmth to the region are common. Clinical examination shows pain to palpation at the retrocalcaneus at a level just before the Achilles tendon. Increase pressure and friction of the Achilles tendon across the retrocalcaneal region is the cause of this bursitis. A high arch, tight Achilles tendon or bone spur appear to be some of the main causes of this problem. With a high arch the back portion of the calcaneus abnormally projects into the Achilles tendon region.
Symptoms
Pain and tenderness are common symptoms. If the affected joint is close to the skin, as with the shoulder, knee, elbow, or Achilles tendon, swelling and redness are seen and the area may feel warm to the touch. The bursae around the hip joint are deeper, and swelling is not obvious. Movement may be limited and is painful. In the shoulder, it may be difficult to raise the arm out from the side of the body. Putting on a jacket or combing the hair becomes a troublesome activity. In acute bursitis symptoms appear suddenly, with chronic bursitis, pain, tenderness, and limited movement reappear after exercise or strain.
Diagnosis
Diagnosis is first by clinical suspicion of symptoms. This can be mistaken for gout or infection especially in the big toe region. A diagnosis of bursitis is usually used in combination of the underlying cause, for instance a bunion deformity, Haglund's deformity, or Heel Spur Syndrome. Many times the cause needs to be addressed to rid the problem of bursitis.
Non Surgical Treatment
Your health care provider may recommend the following treatments. Avoid activities that cause pain. Ice the heel several times a day. Take nonsteroidal anti-inflammatory medications (for example, ibuprofen). Try over-the-counter or custom heel wedges to help decrease the stress on the heel. Try ultrasound treatment during physical therapy to reduce inflammation. Use physical therapy to improve flexibility and strength around the ankle, which can help the bursitis improve and prevent it from coming back. If these treatments don't work, your health care provider may inject a small amount of steroids into the bursa. After the injection, you should avoid stretching the tendon too much because it can break open (rupture). If the condition is connected with Achilles tendinitis, casting the ankle for several weeks to keep it from moving can be effective. Very rarely, surgery may be needed to remove the inflamed bursa.
Prevention
Contact your physician if bursitis pain is disabling (when movement of the joint is largely or entirely restricted), if the pain doesn?t subside after a week of self-care, or if the joint is red and swollen. Also call your doctor if you develop a fever, which could signal infectious bursitis-a condition that especially can afflict the elbow. Except for the fever, symptoms resemble other forms of bursitis, but infectious bursitis requires immediate medical attention.
Hammer Toe Treatment
 Overview
Overview
hammertoes is a painful deformity wherein a toe bends unnaturally and becomes clawlike. This happens because the tendons of the toe contract abnormally, forcing the toe to bend downward and the middle joint of the toe to protrude upward. Although any toe may be affected, hammertoe usually affects the second toe. The toe assumes a clawlike position and cannot be straightened out. When someone with hammertoe wears shoes, the toe is constantly rubbed, so walking may become especially painful if a callus on the sole of the foot or a corn on the top of a toe develops.
Causes
A common cause of hammertoe and mallet toe is wearing improper footwear - shoes that are too tight in the toe box, or high-heel shoes. Wearing shoes of either type can push your toes forward, crowding one or more of them into a space that's not large enough to allow your toes to lie flat. Hammertoe and mallet toe deformities can also be inherited and may occur despite wearing appropriate footwear. The result is a toe that bends upward in the middle and then curls down in a hammer-like or claw-like shape. Your shoes can rub against the raised portion of the toe or toes, causing painful corns or calluses. The bottom of the affected toe can press down, creating the mallet-like appearance of mallet toe. At first, a hammertoe or mallet toe may maintain its flexibility and lie flat when you're not wearing crowded footwear. But eventually, the tendons of the toe may contract and tighten, causing your toe to become permanently stiff.
 Symptoms
Symptoms
The most common symptoms of hammertoes include. The toe is bent upward at the middle toe joint, so that the top of this joint rubs against the top of the shoe. The remainder of the toe is bent downward. Pain upon pressure at the top of the bent toe from footwear. The formation of corns on the top of the joint. Redness and swelling at the joint contracture. Restricted or painful motion of the toe joint. Pain in the ball of the foot at the base of the affected toe. This occurs because the contracted digit puts pressure on the metatarsal head creating callouse and pressure on the ball of the foot.
Diagnosis
The treatment options vary with the type and severity of each hammer toe, although identifying the deformity early in its development is important to avoid surgery. Your podiatric physician will examine and X-ray the affected area hammertoes and recommend a treatment plan specific to your condition.
Non Surgical Treatment
If the problem is caught in the early stages you can avoid hammer toe surgery. One of the easiest methods of treatment is to manipulate the toe out of a bent position then splint and buddy wrap it alongside it?s larger neighbour. This method of hammer toe taping will help the problem to fix itself. Make sure the toe isn?t resuming its bent shape during the recovery. To alleviate some of the painful symptoms of hammer toe avoid wearing high heels or shoes that cramp or stifle your feet. Choosing a pair of minimalist shoes can be an excellent choice for both foot and postural health. Wearing shoes that give the toes plenty of space and are comfortable lined is also a smart choice. Hammer toe recovery starts be treating the toe respectfully. Soft insoles or protection for the corn can also provide additional assistance.
Surgical Treatment
Surgery is used when other types of treatment fail to relieve symptoms or for advanced cases of hammertoe. There are several types of surgeries to treat hammertoe. A small piece of bone may be removed from the joint (arthroplasty). The toe joint may be fused to straighten it (arthrodesis). Surgical hardware, such as a pin, may be used to hold the bones in place while they heal. Other types of surgery involve removing skin (wedging) or correcting muscles and tendons to balance the joint.
Could Cortisone Alleviate Hammer Toe Pain
.jpg) Overview
Overview
A Hammer toe is a contracture, or bending, of the toe at the first joint of the digit, called the proximal interphalangeal joint. This bending causes the toe to appear like an upside-down V when looked at from the side. Any toe can be involved, but the condition usually affects the second through fifth toes, known as the lesser digits. Hammer toes are more common in females than males.
Causes
Hereditary and shoe gear are probably the most likely reasons to develop a hammer toe. Tight pointy shoes may cause a hammer toes. High heels also can cause hammer toes. A deformed toe often develops over time, and certain types of feet may be predisposed. Some patients may develop a hammer toe or cross over toe (of the 2nd toe) due to a bunion of the big toe.
 Symptoms
Symptoms
A hammertoe may be present but not always painful unless irritated by shoes. One may have enlarged toe joints with some thickened skin and no redness or swelling. However, if shoes create pressure on the joint, the pain will usually range from pinching and squeezing to sharp and burning. In long standing conditions, the dislocated joints can cause the pain of arthritis.
Diagnosis
The earlier a hammertoe is diagnosed, the better the prognosis and treatment options. Your doctor will be able to diagnose your hammertoe with a simple examination of the foot and your footwear. He or she may take an x-ray to check the severity of the condition. You may also be asked about your symptoms, your normal daily activities, and your Hammer toes medical and family history.
Non Surgical Treatment
There are many non-surgical treatments to help relieve symptoms of hammertoe. The first step for many people is wearing the right size and type of shoe. Low-heeled shoes with a boxy or roomy toe area are helpful. Cushioned insoles, customized orthopedic inserts, and pads can provided relief as well. Splints or straps may be used to help correct toe position. Your doctor may show you toe stretches and exercises to perform. Your doctor can safely remove corns and calluses. You should not try to remove them at home.
Surgical Treatment
he basis for hammer toe surgery most often involves removing s portion of bone within the toe, to reduce the joint contracture. Depending on the direction the toe is deviated, soft tissue procedures may be necessary along with pinning the toe with a surgical wire.
Bunions Causes Symptoms And Treatments
Overview
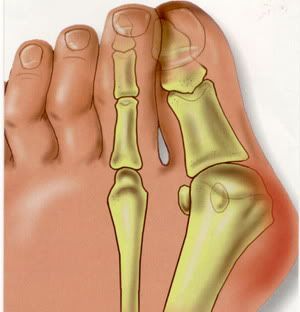 Bunions are one of the most common forefoot deformities. A displacement of the bone under the 1st toe occurs. This causes the big toe to move towards the smaller toes. This shifting of the bones causes a bony prominence on the side of the patients foot (the bunion joint). Over a period of time the big toe may come to rest under (occasionally over) the 2nd toe.
Bunions are one of the most common forefoot deformities. A displacement of the bone under the 1st toe occurs. This causes the big toe to move towards the smaller toes. This shifting of the bones causes a bony prominence on the side of the patients foot (the bunion joint). Over a period of time the big toe may come to rest under (occasionally over) the 2nd toe.
Causes
There are many factors which can contribute to the development of a bunion. The common causes are genetic factors, poor foot mechanics, high-heeled or narrow footwear and trauma to the toe. It is believed that constant stress on the joint of the big toe causes mild displacement of the bones and the joint, along with thickening of the tissues and a change in the pull of the muscles. This can result in a degree of arthritis of the joint, and over time, further displacement of the toe. This may lead to pain, difficultly with fitting shoes and corns/calloused lesions due to excess pressure on the smaller digits.
Symptoms
Audible clicking (called ?crepitus?) and/or stiffness in the affected joint which indicates that the joint surfaces are rubbing together improperly. Inflammation, degeneration of the surfaces of the joint, deformity (including bone growth at the joint line and displacement of the toe) and ultimately, loss of range of motion in the joint. Pain at the side and top of the joint that worsens with walking and physical activity.
Diagnosis
Diagnosis begins with a careful history and physical examination by your doctor. This will usually include a discussion about shoe wear and the importance of shoes in the development and treatment of the condition. X-rays will probably be suggested. This allows your doctor to measure several important angles made by the bones of the feet to help determine the appropriate treatment.
Non Surgical Treatment
A bunion may only need to be treated if it's severe and causing significant pain and discomfort. The different treatments for bunions are described below. If possible, non-surgical treatment for bunions will be used, which your GP can discuss with you. Non-surgical treatments can ease the pain and discomfort caused by a bunion, but they can't change the shape of your foot or prevent a bunion from getting worse over time. Non-surgical treatments include painkillers, bunion pads, orthotics, wearing suitable footwear, These are discussed in more detail below. If your bunion is painful, over-the-counter painkillers such as paracetamol or ibuprofen may be recommended.Bunion pads may also ease the pain of a bunion. Reusable bunion pads, made of either gel or fleece, are available over the counter from pharmacies. Some are adhesive and stick over the bunion, while others are held against your foot by a small loop that fits over your big toe. Bunion pads stop your foot rubbing on your shoe and relieve the pressure over the enlarged joint at the base of your big toe. Orthotics are placed inside your shoes to help realign the bones of your foot. They may help relieve the pressure on your bunion, which can ease the pain. However, there's little evidence that orthotics are effective in the long term. It's important that the orthotic fits properly, so you may want to seek advice from your GP or podiatrist (a specialist in diagnosing and treating foot conditions), who can suggest the best ones for you. 
Surgical Treatment
Surgery takes place either under local or general anaesthetic and takes about one hour. After surgery you will have either a plaster cast or special dressing on the foot and you will be given a special walking shoe and crutches to use the first few days/weeks. Recovery usually takes approximately 6-8 weeks but swelling often lasts longer and it may take a few months before you are able to wear normal shoes again. Full recovery can take up to a year. Bunion surgery is successful in approximately 85% of cases, but it is vital not to go back to wearing ill-fitting shoes else the problem is likely to return.
The Causes And Treatment Of Over-Pronation
Overview
Over-pronation is very common and affects millions of people. To better understand this condition, we'll take a closer look at the 3 most common foot types. An estimated 70% of the population has fallen arches (or a low arch). Only 20% has a normal arch. And 10% have abnormal feet, in other words they either have flat feet or the opposite a high arched foot.
Causes
Overpronation often occurs in people with flat feet, whose plantar fascia ligament is too flexible or too long, and therefore unable to properly support the longitudinal arch of the foot. People tend to inherit the foot structure that leads to overpronation. In a normal foot the bones are arranged so that two arches are formed, the longitudinal and the transverse. Ligaments hold all the bones in their correct positions, and tendons attach muscles to bones. If the bones are held together too loosely, they will tend to move inwards as this is the easiest direction for them to go. Over time the soft tissue structures will adjust to the misalignment and the foot will become permanently over-flexible, with a flat arch.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
Pronounced wear on the instep side of shoe heels can indicate overpronation, however it's best to get an accurate assessment. Footbalance retailers offer a free foot analysis to check for overpronation and help you learn more about your feet.
Non Surgical Treatment
Overpronation is usually corrected with orthotics and/or strengthening exercises for the tibialis posterior. Massage treatment can relieve myofascial trigger points in the tibialis posterior, and other muscles, and address any resulting neuromuscular dysfunction in the leg or foot. Biomechanical correction of overpronation might require orthotics, neuromuscular reeducation, or gait retraining methods, as well. Stretching the gastrocnemius and soleus muscles will reduce hypertonicity in these muscles and also is essential for effective treatment. Because of impacts throughout the remainder of the body, the detrimental effects of overpronation should not be overlooked.
Prevention
Pronation forces us to bear most of our weight on the inner border of our feet. Custom-made orthotics gently redistributes the weight so that the entire foot bears its normal share of weight with each step we take. The foot will not twist out at the ankle, but will strike the ground normally when the orthotics is used. This action of the custom-made orthotics will help to prevent shin splints, ankle sprains, knee and hip pain, lower back pain, nerve entrapments, tendonitis, muscle aches, bunions, generalized fatigue, hammer toes, and calluses.
Over-pronation is very common and affects millions of people. To better understand this condition, we'll take a closer look at the 3 most common foot types. An estimated 70% of the population has fallen arches (or a low arch). Only 20% has a normal arch. And 10% have abnormal feet, in other words they either have flat feet or the opposite a high arched foot.
Causes
Overpronation often occurs in people with flat feet, whose plantar fascia ligament is too flexible or too long, and therefore unable to properly support the longitudinal arch of the foot. People tend to inherit the foot structure that leads to overpronation. In a normal foot the bones are arranged so that two arches are formed, the longitudinal and the transverse. Ligaments hold all the bones in their correct positions, and tendons attach muscles to bones. If the bones are held together too loosely, they will tend to move inwards as this is the easiest direction for them to go. Over time the soft tissue structures will adjust to the misalignment and the foot will become permanently over-flexible, with a flat arch.
Symptoms
Overpronation can lead to injuries and pain in the foot, ankle, knee, or hip. Overpronation puts extra stress on all the bones in the feet. The repeated stress on the knees, shins, thighs, and pelvis puts additional stress on the muscles, tendons, and ligaments of the lower leg. This can put the knee, hip, and back out of alignment, and it can become very painful.
Diagnosis
Pronounced wear on the instep side of shoe heels can indicate overpronation, however it's best to get an accurate assessment. Footbalance retailers offer a free foot analysis to check for overpronation and help you learn more about your feet.
Non Surgical Treatment
Overpronation is usually corrected with orthotics and/or strengthening exercises for the tibialis posterior. Massage treatment can relieve myofascial trigger points in the tibialis posterior, and other muscles, and address any resulting neuromuscular dysfunction in the leg or foot. Biomechanical correction of overpronation might require orthotics, neuromuscular reeducation, or gait retraining methods, as well. Stretching the gastrocnemius and soleus muscles will reduce hypertonicity in these muscles and also is essential for effective treatment. Because of impacts throughout the remainder of the body, the detrimental effects of overpronation should not be overlooked.
Prevention
Pronation forces us to bear most of our weight on the inner border of our feet. Custom-made orthotics gently redistributes the weight so that the entire foot bears its normal share of weight with each step we take. The foot will not twist out at the ankle, but will strike the ground normally when the orthotics is used. This action of the custom-made orthotics will help to prevent shin splints, ankle sprains, knee and hip pain, lower back pain, nerve entrapments, tendonitis, muscle aches, bunions, generalized fatigue, hammer toes, and calluses.
Does Calcaneal Apophysitis Necessitate Surgical Procedures?
Overview
Sever disease, first described in 1912, is a painful inflammation of the calcaneal apophysis. It is classified with the child and adolescent nonarticular osteochondroses. (The other disease in this group is Iselin disease, which is inflammation of the base of the fifth metatarsal.) The etiology of pain in Sever disease is believed to be repetitive trauma to the weaker structure of the apophysis, induced by the pull of the tendo calcaneus (Achilles tendon) on its insertion. This results in a clinical picture of heel pain in a growing active child, which worsens with activity. Sever disease is a self-limited condition; accordingly, no known complication exists from failure to make the correct diagnosis.
Causes
This condition is more common in boys than girls. It generally presents between the ages of 9-14 and peaks between ages 10-12 years. This injury can reoccur up until the age of 17, when the growth plate of the calcaneous generally closes. These types of injuries will commonly occur during periods of rapid growth. Sever?s Disease occurs more frequently in child with flat feet, but all children with flat feet will not get Sever?s.
Symptoms
Pain symptoms usually begin after a child begins a new sport or sporting season, and can worsen with athletic activities that involve running and jumping. It is common for a child with Sever?s disease to walk with a limp. Increased activity can lead to heel cord tightness (Achilles Tendon), resulting in pressure on the apophysis of the calcaneus. This will cause irritation of the growth plate and sometimes swelling in the heel area thus producing pain. This usually occurs in the early stages of puberty.
Diagnosis
A physical exam of the heel will show tenderness over the back of the heel but not in the Achilles tendon or plantar fascia. There may be tightness in the calf muscle, which contributes to tension on the heel. The tendons in the heel get stretched more in patients with flat feet. There is greater impact force on the heels of athletes with a high-arched, rigid foot. The doctor may order an x-ray because x-rays can confirm how mature the growth center is and if there are other sources of heel pain, such as a stress fracture or bone cyst. However, x-rays are not necessary to diagnose Sever?s disease, and it is not possible to make the diagnosis based on the x-ray alone.
Non Surgical Treatment
The aim of treatment is to reduce the pain and inflammation when gently stretch the muscles. There is likely to be no magic instant cure and the young athlete may have to be patient while they grow. Rest and apply ice or cold therapy to the heel. Do not apply ice directly to the skin but wrap in a wet tea towel to avoid ice burns. Rest from activities which cause pain. If running and playing football makes it worse then reduce or stop this activity and try cycling or swimming to maintain fitness. A temporary measure is to insert a heel pad or heel raise into the shoes. This has the effect of raising the heel and shortening the calf muscles and so taking the strain off the back of the heel. However long term use of a heal raise may shorten the calf muscles when they need stretching. Stretch the calf muscles regularly. Stretching should be done pain free and very gently with this injury. See a sports injury professional who can advise on treatment and rehabilitation.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position. If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
Sever disease, first described in 1912, is a painful inflammation of the calcaneal apophysis. It is classified with the child and adolescent nonarticular osteochondroses. (The other disease in this group is Iselin disease, which is inflammation of the base of the fifth metatarsal.) The etiology of pain in Sever disease is believed to be repetitive trauma to the weaker structure of the apophysis, induced by the pull of the tendo calcaneus (Achilles tendon) on its insertion. This results in a clinical picture of heel pain in a growing active child, which worsens with activity. Sever disease is a self-limited condition; accordingly, no known complication exists from failure to make the correct diagnosis.
Causes
This condition is more common in boys than girls. It generally presents between the ages of 9-14 and peaks between ages 10-12 years. This injury can reoccur up until the age of 17, when the growth plate of the calcaneous generally closes. These types of injuries will commonly occur during periods of rapid growth. Sever?s Disease occurs more frequently in child with flat feet, but all children with flat feet will not get Sever?s.
Symptoms
Pain symptoms usually begin after a child begins a new sport or sporting season, and can worsen with athletic activities that involve running and jumping. It is common for a child with Sever?s disease to walk with a limp. Increased activity can lead to heel cord tightness (Achilles Tendon), resulting in pressure on the apophysis of the calcaneus. This will cause irritation of the growth plate and sometimes swelling in the heel area thus producing pain. This usually occurs in the early stages of puberty.
Diagnosis
A physical exam of the heel will show tenderness over the back of the heel but not in the Achilles tendon or plantar fascia. There may be tightness in the calf muscle, which contributes to tension on the heel. The tendons in the heel get stretched more in patients with flat feet. There is greater impact force on the heels of athletes with a high-arched, rigid foot. The doctor may order an x-ray because x-rays can confirm how mature the growth center is and if there are other sources of heel pain, such as a stress fracture or bone cyst. However, x-rays are not necessary to diagnose Sever?s disease, and it is not possible to make the diagnosis based on the x-ray alone.
Non Surgical Treatment
The aim of treatment is to reduce the pain and inflammation when gently stretch the muscles. There is likely to be no magic instant cure and the young athlete may have to be patient while they grow. Rest and apply ice or cold therapy to the heel. Do not apply ice directly to the skin but wrap in a wet tea towel to avoid ice burns. Rest from activities which cause pain. If running and playing football makes it worse then reduce or stop this activity and try cycling or swimming to maintain fitness. A temporary measure is to insert a heel pad or heel raise into the shoes. This has the effect of raising the heel and shortening the calf muscles and so taking the strain off the back of the heel. However long term use of a heal raise may shorten the calf muscles when they need stretching. Stretch the calf muscles regularly. Stretching should be done pain free and very gently with this injury. See a sports injury professional who can advise on treatment and rehabilitation.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position. If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
Causes Of Acquired Flat Foot
Overview
Many foot problems can be contributed to Adult Acquired Flatfoot Deformity (AAFD), a foot and ankle condition that causes fallen arch of the foot. AAFD is also referred to as Posterior Tibial Tendon Dysfunction (PTTD). The posterior tibial tendon serves as the principal supporting structure of your foot. When this ligament is injured overtime the arches start to flatten, leaving you with a painful foot condition. AAFD is more common in women ages 39 - 65 than men. 
Causes
The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction. What causes adult acquired flat foot? Fracture or dislocation. Tendon laceration. Tarsal Coalition. Arthritis. Neuroarthropathy. Neurological weakness.
Symptoms
Patients often experience pain and/or deformity at the ankle or hindfoot. When the posterior tibial tendon does not work properly, a number of changes can occur to the foot and ankle. In the earlier stages, symptoms often include pain and tenderness along the posterior tibial tendon behind the inside of the ankle. As the tendon progressively fails, deformity of the foot and ankle may occur. This deformity can include progressive flattening of the arch, shifting of the heel so that it no longer is aligned underneath the rest of the leg, rotation and deformity of the forefoot, tightening of the heel cord, development of arthritis, and deformity of the ankle joint. At certain stages of this disorder, pain may shift from the inside to the outside aspect of the ankle as the heel shifts outward and structures are pinched laterally.
Diagnosis
The history and physical examination are probably the most important tools the physician uses to diagnose this problem. The wear pattern on your shoes can offer some helpful clues. Muscle testing helps identify any areas of weakness or muscle impairment. This should be done in both the weight bearing and nonweight bearing positions. A very effective test is the single heel raise. You will be asked to stand on one foot and rise up on your toes. You should be able to lift your heel off the ground easily while keeping the calcaneus (heel bone) in the middle with slight inversion (turned inward). X-rays are often used to study the position, shape, and alignment of the bones in the feet and ankles. Magnetic resonance (MR) imaging is the imaging modality of choice for evaluating the posterior tibial tendon and spring ligament complex.
Non surgical Treatment
A patient who has acute tenosynovitis has pain and swelling along the medial aspect of the ankle. The patient is able to perform a single-limb heel-rise test but has pain when doing so. Inversion of the foot against resistance is painful but still strong. The patient should be managed with rest, the administration of appropriate anti-inflammatory medication, and immobilization. The injection of corticosteroids is not recommended. Immobilization with either a rigid below-the-knee cast or a removable cast or boot may be used to prevent overuse and subsequent rupture of the tendon. A removable stirrup-brace is not initially sufficient as it does not limit motion in the sagittal plane, a component of the pathological process. The patient should be permitted to walk while wearing the cast or boot during the six to eight-week period of immobilization. At the end of that time, a decision must be made regarding the need for additional treatment. If there has been marked improvement, the patient may begin wearing a stiff-soled shoe with a medial heel-and-sole wedge to invert the hindfoot. If there has been only mild or moderate improvement, a longer period in the cast or boot may be tried. 
Surgical Treatment
The indications for surgery are persistent pain and/or significant deformity. Sometimes the foot just feels weak and the assessment of deformity is best done by a foot and ankle specialist. If surgery is appropriate, a combination of soft tissue and bony procedures may be considered to correct alignment and support the medial arch, taking strain off failing ligaments. Depending upon the tissues involved and extent of deformity, the foot and ankle specialist will determine the necessary combination of procedures. Surgical procedures may include a medial slide calcaneal osteotomy to correct position of the heel, a lateral column lengthening to correct position in the midfoot and a medial cuneiform osteotomy or first metatarsal-tarsal fusion to correct elevation of the medial forefoot. The posterior tibial tendon may be reconstructed with a tendon transfer. In severe cases (stage III), the reconstruction may include fusion of the hind foot,, resulting in stiffness of the hind foot but the desired pain relief. In the most severe stage (stage IV), the deltoid ligament on the inside of the ankle fails, resulting in the deformity in the ankle. This deformity over time can result in arthritis in the ankle.