A Way To Diagnose Fallen Arches
Overview

Some people have always had flat feet from a young age. Unfortunately as people reach their fifties they will suddenly have one foot with a flatter arch than the other foot. This situation is termed adult acquired flatfoot. Adult acquired flatfoot is a painful condition occurring in one foot. The common patient profile is a female over the age of 50 with pre-existing flatfeet, high blood pressure, high cholesterol, diabetes and obesity. All of these underlying problems will lead to a weakening of the support structures of the arch. If you have adult acquired flat foot you will not be able to lift your heel off the ground while standing on one leg. Adult acquired flatfoot may develop due to trauma or degeneration of major tendons ankle & foot. Weakness or paralysis of leg muscles can also create a flatfoot deformity. Adult acquired flat foot can be treated with physical therapies, motion control running shoes or hiking boots, custom foot orthoses, and ankle foot orthoses.
Causes
Some people develop fallen arches because they tend to pronate, or roll inwards on the ankles, says the Instep Foot Clinic. Other people may simply have under-developed muscles in their arches. Your arches help your feet bear weight and are supported in this job by muscles and tendons in your feet and ankles. So, while fallen arches aren?t usually serious, they can cause pain in your feet, ankles, knees and/or hips due to your reduced weight-bearing ability. In these cases, treatment may be required. Orthotics that sit in your shoes and support your arches are a common solution, as are exercises to strengthen and stretch your feet and leg muscles.
Symptoms
Having flat feet can be painless and is actually normal in some people. But others with flat feet experience pain in the heel or arch area, difficulty standing on tiptoe, or have swelling along the inside of the ankle. They may also experience pain after standing for long periods of time or playing sports. Some back problems can also be attributed to flat feet.
Diagnosis
If your child has flatfeet, his or her doctor will ask about any family history of flatfeet or inherited foot problems. In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics. The doctor will examine your feet for foot flexibility and range of motion and feel for any tenderness or bony abnormalities. Depending on the results of this physical examination, foot X-rays may be recommended. X-rays are always performed in a young child with rigid flatfeet and in an adult with acquired flatfeet due to trauma.
heelsncleavage
Non Surgical Treatment
What we want to do is support the arch and maintain it in that curved position. So what you want is to bring the foot into a position where you hold and support the arch so you can get that correct heel-midfoot-big toe contact. You would achieve that with a level of arch support. People will take different levels of support, if you?re somebody who has movement in your arch, a strong level of support will hold and maintain you whereas if you?re someone whose arch has collapsed it could need more support and a level of correction built into the support to realign you. If you think of it, when your arch drops, it affects your foot but it also has a biomechanical effect on the rest of the body. But nothing that can?t be solved.
Surgical Treatment

This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients.
Prevention
Orthotic inserts, either prescribed or bought over the counter, can help keep the arches fixed into position, but always wear them as although they support, they don?t strengthen, which is why some experts reccomend avoiding them. Gait analysis at a run specialist can help to diagnose overpronation and flat feet. Most brands produce shoes that will give support and help to limit the negative effects of a poor gait on the rest of the body. Barefoot exercises, such as standing on a towel and making fists with the toes, can help to strengthen the arches. Start easy and build up the reps to avoid cramping. Short barefoot running sessions can help take pressure off the arches by using the natural elasticity of the foot?s tendons to take impact and build strength to help prevent flat feet. These should be done on grass for only a few minutes at a time.
Some people have always had flat feet from a young age. Unfortunately as people reach their fifties they will suddenly have one foot with a flatter arch than the other foot. This situation is termed adult acquired flatfoot. Adult acquired flatfoot is a painful condition occurring in one foot. The common patient profile is a female over the age of 50 with pre-existing flatfeet, high blood pressure, high cholesterol, diabetes and obesity. All of these underlying problems will lead to a weakening of the support structures of the arch. If you have adult acquired flat foot you will not be able to lift your heel off the ground while standing on one leg. Adult acquired flatfoot may develop due to trauma or degeneration of major tendons ankle & foot. Weakness or paralysis of leg muscles can also create a flatfoot deformity. Adult acquired flat foot can be treated with physical therapies, motion control running shoes or hiking boots, custom foot orthoses, and ankle foot orthoses.
Causes
Some people develop fallen arches because they tend to pronate, or roll inwards on the ankles, says the Instep Foot Clinic. Other people may simply have under-developed muscles in their arches. Your arches help your feet bear weight and are supported in this job by muscles and tendons in your feet and ankles. So, while fallen arches aren?t usually serious, they can cause pain in your feet, ankles, knees and/or hips due to your reduced weight-bearing ability. In these cases, treatment may be required. Orthotics that sit in your shoes and support your arches are a common solution, as are exercises to strengthen and stretch your feet and leg muscles.
Symptoms
Having flat feet can be painless and is actually normal in some people. But others with flat feet experience pain in the heel or arch area, difficulty standing on tiptoe, or have swelling along the inside of the ankle. They may also experience pain after standing for long periods of time or playing sports. Some back problems can also be attributed to flat feet.
Diagnosis
If your child has flatfeet, his or her doctor will ask about any family history of flatfeet or inherited foot problems. In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics. The doctor will examine your feet for foot flexibility and range of motion and feel for any tenderness or bony abnormalities. Depending on the results of this physical examination, foot X-rays may be recommended. X-rays are always performed in a young child with rigid flatfeet and in an adult with acquired flatfeet due to trauma.
heelsncleavage
Non Surgical Treatment
What we want to do is support the arch and maintain it in that curved position. So what you want is to bring the foot into a position where you hold and support the arch so you can get that correct heel-midfoot-big toe contact. You would achieve that with a level of arch support. People will take different levels of support, if you?re somebody who has movement in your arch, a strong level of support will hold and maintain you whereas if you?re someone whose arch has collapsed it could need more support and a level of correction built into the support to realign you. If you think of it, when your arch drops, it affects your foot but it also has a biomechanical effect on the rest of the body. But nothing that can?t be solved.
Surgical Treatment
This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients.
Prevention
Orthotic inserts, either prescribed or bought over the counter, can help keep the arches fixed into position, but always wear them as although they support, they don?t strengthen, which is why some experts reccomend avoiding them. Gait analysis at a run specialist can help to diagnose overpronation and flat feet. Most brands produce shoes that will give support and help to limit the negative effects of a poor gait on the rest of the body. Barefoot exercises, such as standing on a towel and making fists with the toes, can help to strengthen the arches. Start easy and build up the reps to avoid cramping. Short barefoot running sessions can help take pressure off the arches by using the natural elasticity of the foot?s tendons to take impact and build strength to help prevent flat feet. These should be done on grass for only a few minutes at a time.
Do You Understand Heel Aches?
Overview

The heel is a padded cushion of fatty tissue around the heel bone (the calcaneus) that holds its shape despite the pressure of body weight and movement. It serves to protect the structures of the foot, including the calcaneus, muscles and ligaments. Heel pain is a very common foot complaint. Anyone can suffer from heel pain, but certain groups seem to be at increased risk, including Middle-aged men and women, Physically active people, People who are overweight or obese, People who are on their feet for long periods of time, Children aged between eight and 13 years (particularly boys), Women during pregnancy.
Causes
Pain in the foot can be due to a problem in any part of the foot. Bones, ligaments, tendons, muscles, fascia, toenail beds, nerves, blood vessels, or skin can be the source of foot pain. The cause of foot pain can be narrowed down by location and by considering some of the most common causes of foot pain. Plantar fasciitis is the most common cause of heel pain. The plantar fascia, a band of tough tissue connecting the heel bone to the toes, becomes irritated or inflamed. Heel pain, worst in the morning when getting out of bed, is the most common symptom. Arch pain may also be present.
Symptoms
Usually worse with the first few steps in the morning or at the initial point of activity. The latter usually gets better with continued activity (squeaky hinge analogy). Walking, running, sprinting, hill running and jumping will increase the pain. Often, the natural response is to walk on the outside of the foot - in supination - to lessen the stress on the plantar fascia - resulting in new problems.
Diagnosis
After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests.
Non Surgical Treatment
Shoes, orthoses, splinting and/or immobilization form the cornerstone for successful functional management of plantar fasciitis.When you take the overuse nature of plantar fasciitis into account and attempt to re-establish the windlass mechanism of the foot, there is an enhanced potential for success. Unfortunately, too little attention has been directed to appropriately managing the shoes worn during treatment for plantar fasciitis. Emphasising motion control and stability type athletic shoes (that provide a firm heel cup, instep rigidity, longitudinal integrity and a well-integrated shoe upper) can help decrease excess eccentric tissue strain. The shoe also serves as a vital and functional link between an orthotic and the foot. Orthoses have long been considered to be a reliable method for treating plantar fasciitis. Considerable debate has been waged over the benefits of over-the-counter (OTC), prefabricated and prescription foot and/or ankle orthoses. Heel cushions, heel cups and cushioning pads appear to provide immediate pain relief for many people who have plantar fasciitis.This relief is frequently short-lived and requires other treatment modalities for success.Neutral position taping and strapping of the foot provides temporary symptomatic relief of pain caused by plantar fasciitis. Although the functional benefits are temporary and likely do not last longer than 10 minutes with exercise, the soft tissue compression and symptomatic relief afforded by the strapping can last for nearly a week.
Surgical Treatment
Surgery is a last resort in the treatment of heel pain. Physicians have developed many procedures in the last 100 years to try to cure heel pain. Most procedures that are commonly used today focus on several areas, remove the bone spur (if one is present), release the plantar fascia (plantar fasciotomy), release pressure on the small nerves in the area. Usually the procedure is done through a small incision on the inside edge of the foot, although some surgeons now perform this type of surgery using an endoscope. An endoscope is a tiny TV camera that can be inserted into a joint or under the skin to allow the surgeon to see the structures involved in the surgery. By using the endoscope, a surgeon can complete the surgery with a smaller incision and presumably less damage to normal tissues. It is unclear whether an endoscopic procedure for this condition is better than the traditional small incision. Surgery usually involves identifying the area where the plantar fascia attaches to the heel and releasing the fascia partially from the bone. If a small spur is present this is removed. The small nerves that travel under the plantar fascia are identified and released from anything that seems to be causing pressure on the nerves. This surgery can usually be done on an outpatient basis. This means you can leave the hospital the same day.
heel pain cure
Prevention

A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don?t underestimate your body's need for rest and good nutrition. If obese, lose weight.
The heel is a padded cushion of fatty tissue around the heel bone (the calcaneus) that holds its shape despite the pressure of body weight and movement. It serves to protect the structures of the foot, including the calcaneus, muscles and ligaments. Heel pain is a very common foot complaint. Anyone can suffer from heel pain, but certain groups seem to be at increased risk, including Middle-aged men and women, Physically active people, People who are overweight or obese, People who are on their feet for long periods of time, Children aged between eight and 13 years (particularly boys), Women during pregnancy.
Causes
Pain in the foot can be due to a problem in any part of the foot. Bones, ligaments, tendons, muscles, fascia, toenail beds, nerves, blood vessels, or skin can be the source of foot pain. The cause of foot pain can be narrowed down by location and by considering some of the most common causes of foot pain. Plantar fasciitis is the most common cause of heel pain. The plantar fascia, a band of tough tissue connecting the heel bone to the toes, becomes irritated or inflamed. Heel pain, worst in the morning when getting out of bed, is the most common symptom. Arch pain may also be present.
Symptoms
Usually worse with the first few steps in the morning or at the initial point of activity. The latter usually gets better with continued activity (squeaky hinge analogy). Walking, running, sprinting, hill running and jumping will increase the pain. Often, the natural response is to walk on the outside of the foot - in supination - to lessen the stress on the plantar fascia - resulting in new problems.
Diagnosis
After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests.
Non Surgical Treatment
Shoes, orthoses, splinting and/or immobilization form the cornerstone for successful functional management of plantar fasciitis.When you take the overuse nature of plantar fasciitis into account and attempt to re-establish the windlass mechanism of the foot, there is an enhanced potential for success. Unfortunately, too little attention has been directed to appropriately managing the shoes worn during treatment for plantar fasciitis. Emphasising motion control and stability type athletic shoes (that provide a firm heel cup, instep rigidity, longitudinal integrity and a well-integrated shoe upper) can help decrease excess eccentric tissue strain. The shoe also serves as a vital and functional link between an orthotic and the foot. Orthoses have long been considered to be a reliable method for treating plantar fasciitis. Considerable debate has been waged over the benefits of over-the-counter (OTC), prefabricated and prescription foot and/or ankle orthoses. Heel cushions, heel cups and cushioning pads appear to provide immediate pain relief for many people who have plantar fasciitis.This relief is frequently short-lived and requires other treatment modalities for success.Neutral position taping and strapping of the foot provides temporary symptomatic relief of pain caused by plantar fasciitis. Although the functional benefits are temporary and likely do not last longer than 10 minutes with exercise, the soft tissue compression and symptomatic relief afforded by the strapping can last for nearly a week.
Surgical Treatment
Surgery is a last resort in the treatment of heel pain. Physicians have developed many procedures in the last 100 years to try to cure heel pain. Most procedures that are commonly used today focus on several areas, remove the bone spur (if one is present), release the plantar fascia (plantar fasciotomy), release pressure on the small nerves in the area. Usually the procedure is done through a small incision on the inside edge of the foot, although some surgeons now perform this type of surgery using an endoscope. An endoscope is a tiny TV camera that can be inserted into a joint or under the skin to allow the surgeon to see the structures involved in the surgery. By using the endoscope, a surgeon can complete the surgery with a smaller incision and presumably less damage to normal tissues. It is unclear whether an endoscopic procedure for this condition is better than the traditional small incision. Surgery usually involves identifying the area where the plantar fascia attaches to the heel and releasing the fascia partially from the bone. If a small spur is present this is removed. The small nerves that travel under the plantar fascia are identified and released from anything that seems to be causing pressure on the nerves. This surgery can usually be done on an outpatient basis. This means you can leave the hospital the same day.
heel pain cure
Prevention
A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don?t underestimate your body's need for rest and good nutrition. If obese, lose weight.
Apparent Leg Length Discrepancy Following Hip Replacement
Overview
Differences of an inch-and-a-half to two inches may require epiphysiodesis (adjusting the growth of the longer side) or acute shortening of the other side. Differences greater than 2.5 inches usually require a lengthening procedure. The short bone is cut and an external device is applied. Gradual lengthening is done over months to allow the muscles and nerves accommodate the new length.
Causes
Some children are born with absence or underdeveloped bones in the lower limbs e.g., congenital hemimelia. Others have a condition called hemihypertrophy that causes one side of the body to grow faster than the other. Sometimes, increased blood flow to one limb (as in a hemangioma or blood vessel tumor) stimulates growth to the limb. In other cases, injury or infection involving the epiphyseal plate (growth plate) of the femur or tibia inhibits or stops altogether the growth of the bone. Fractures healing in an overlapped position, even if the epiphyseal plate is not involved, can also cause limb length discrepancy. Neuromuscular problems like polio can also cause profound discrepancies, but thankfully, uncommon. Lastly, Wilms? tumor of the kidney in a child can cause hypertrophy of the lower limb on the same side. It is therefore important in a young child with hemihypertrophy to have an abdominal ultrasound exam done to rule out Wilms? tumor. It is important to distinguish true leg length discrepancy from apparent leg length discrepancy. Apparent discrepancy is due to an instability of the hip, that allows the proximal femur to migrate proximally, or due to an adduction or abduction contracture of the hip that causes pelvic obliquity, so that one hip is higher than the other. When the patient stands, it gives the impression of leg length discrepancy, when the problem is actually in the hip.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
A systematic and well organized approach should be used in the diagnosis of LLD to ensure all relevant factors are considered and no clues are overlooked which could explain the difference. To determine the asymmetry a patient should be evaluated whilst standing and walking. During the process special care should be used to note the extent of pelvic shift from side to side and deviation along the plane of the front or leading leg as well as the traverse deviation of the back leg and abnormal curvature of the spine. Dynamic gait analysis should be conducted during waling where observation of movement on the sagittal, frontal and transverse planes should be noted. Also observe head, neck and shoulder movements for any tilting.
Non Surgical Treatment
Heel lifts and sole lifts are simple ways Pedorthists can compensate for leg length deficiencies. These small modifications can make a tremendous difference to a person?s comfort, balance and mobility. Although people do not always know if they have LLD if you have any of the symptoms I have mentioned you should consult a Pedorthist as treating your condition early will reduce the development of serious problems later on.

how we can increase our height?
Surgical Treatment
Surgery is another option. In some cases the longer extremity can be shortened, but a major shortening may weaken the muscles of the extremity. In growing children, lower extremities can also be equalized by a surgical procedure that stops the growth at one or two sites of the longer extremity, while leaving the remaining growth undisturbed. Your physician can tell you how much equalization can be attained by surgically halting one or more growth centers. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the LLD will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical; the goal is to attain equal length of the extremities at skeletal maturity, usually in the mid- to late teens. Disadvantages of this option include the possibility of slight over-correction or under-correction of the LLD and the patient?s adult height will be less than if the shorter extremity had been lengthened. Correction of significant LLDs by this method may make a patient?s body look slightly disproportionate because of the shorter legs.
Differences of an inch-and-a-half to two inches may require epiphysiodesis (adjusting the growth of the longer side) or acute shortening of the other side. Differences greater than 2.5 inches usually require a lengthening procedure. The short bone is cut and an external device is applied. Gradual lengthening is done over months to allow the muscles and nerves accommodate the new length.
Causes
Some children are born with absence or underdeveloped bones in the lower limbs e.g., congenital hemimelia. Others have a condition called hemihypertrophy that causes one side of the body to grow faster than the other. Sometimes, increased blood flow to one limb (as in a hemangioma or blood vessel tumor) stimulates growth to the limb. In other cases, injury or infection involving the epiphyseal plate (growth plate) of the femur or tibia inhibits or stops altogether the growth of the bone. Fractures healing in an overlapped position, even if the epiphyseal plate is not involved, can also cause limb length discrepancy. Neuromuscular problems like polio can also cause profound discrepancies, but thankfully, uncommon. Lastly, Wilms? tumor of the kidney in a child can cause hypertrophy of the lower limb on the same side. It is therefore important in a young child with hemihypertrophy to have an abdominal ultrasound exam done to rule out Wilms? tumor. It is important to distinguish true leg length discrepancy from apparent leg length discrepancy. Apparent discrepancy is due to an instability of the hip, that allows the proximal femur to migrate proximally, or due to an adduction or abduction contracture of the hip that causes pelvic obliquity, so that one hip is higher than the other. When the patient stands, it gives the impression of leg length discrepancy, when the problem is actually in the hip.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
A systematic and well organized approach should be used in the diagnosis of LLD to ensure all relevant factors are considered and no clues are overlooked which could explain the difference. To determine the asymmetry a patient should be evaluated whilst standing and walking. During the process special care should be used to note the extent of pelvic shift from side to side and deviation along the plane of the front or leading leg as well as the traverse deviation of the back leg and abnormal curvature of the spine. Dynamic gait analysis should be conducted during waling where observation of movement on the sagittal, frontal and transverse planes should be noted. Also observe head, neck and shoulder movements for any tilting.
Non Surgical Treatment
Heel lifts and sole lifts are simple ways Pedorthists can compensate for leg length deficiencies. These small modifications can make a tremendous difference to a person?s comfort, balance and mobility. Although people do not always know if they have LLD if you have any of the symptoms I have mentioned you should consult a Pedorthist as treating your condition early will reduce the development of serious problems later on.
how we can increase our height?
Surgical Treatment
Surgery is another option. In some cases the longer extremity can be shortened, but a major shortening may weaken the muscles of the extremity. In growing children, lower extremities can also be equalized by a surgical procedure that stops the growth at one or two sites of the longer extremity, while leaving the remaining growth undisturbed. Your physician can tell you how much equalization can be attained by surgically halting one or more growth centers. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the LLD will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical; the goal is to attain equal length of the extremities at skeletal maturity, usually in the mid- to late teens. Disadvantages of this option include the possibility of slight over-correction or under-correction of the LLD and the patient?s adult height will be less than if the shorter extremity had been lengthened. Correction of significant LLDs by this method may make a patient?s body look slightly disproportionate because of the shorter legs.
Mortons Neuroma Symptoms
Overview
 A neuroma develops when a nerve is compressed, injured or pinched, causing swelling and pain. A neuroma in the area between the third and fourth toes, or between the second and third toes, is known as a Morton?s neuroma. Morton?s neuroma causes sharp, burning pain and numbness in the toes and foot. You may feel like you?ve stepped on a tiny hot coal and can?t get rid of it. At the same time, you?ll have the disconcerting experience of not being able to feel your toes. Sometimes the nerve tissue becomes so thickened you can feel or see a lump.
A neuroma develops when a nerve is compressed, injured or pinched, causing swelling and pain. A neuroma in the area between the third and fourth toes, or between the second and third toes, is known as a Morton?s neuroma. Morton?s neuroma causes sharp, burning pain and numbness in the toes and foot. You may feel like you?ve stepped on a tiny hot coal and can?t get rid of it. At the same time, you?ll have the disconcerting experience of not being able to feel your toes. Sometimes the nerve tissue becomes so thickened you can feel or see a lump.
Causes
Various factors have been implicated in the precipitation of Morton's neuroma. Morton's neuroma is known to develop as a result of chronic nerve stress and irritation, particularly with excessive toe dorsiflexion. Poorly fitting and constricting shoes (ie, small toe box) or shoes with heel lifts often contribute to Morton's neuroma. Women who wear high-heeled shoes for a number of years or men who are required to wear constrictive shoe gear are at risk. A biomechanical theory of causation involves the mechanics of the foot and ankle. For instance, individuals with tight gastrocnemius-soleus muscles or who excessively pronate the foot may compensate by dorsiflexion of the metatarsals subsequently irritating of the interdigital nerve. Certain activities carry increased risk of excessive toe dorsiflexion, such as prolonged walking, running, squatting, and demi-pointe position in ballet.
Symptoms
Symptoms associated with a neuroma include a dull burning sensation radiating towards the toes, a cramping feeling, or even a stinging, tingling sensation that can be described as being similar to an electric shock. It is often worse when wearing shoes with most people finding the pain disappears when removing their shoes.
Diagnosis
To diagnose Morton's neuroma the podiatrist commonly palpates the area to elicit pain, squeezing the toes from the side. Next he or she may try to feel the neuroma by pressing a thumb into the third interspace. The podiatrist then tries to elicit Mulder's sign, by palpating the affected interspace with one hand and squeezing the entire foot at the same time with the other hand. In many cases of Morton's neuroma, this causes an audible click, known as Mulder's sign. An x-ray should be taken to ensure that there is not a fracture. X-rays also can be used to examine the joints and bone density, ruling out arthritis (particularly rheumatoid arthritis and osteoarthritis).
Non Surgical Treatment
The first line of treatment is to try modifying footwear. Often simply wearing broader fitting shoes can reduce pressure on the neuroma and so reduce pain. Orthotic inserts can also help as they can again help reduce pressure on certain parts of the foot. Padding and taping the toe area is another option. In some cases a steroid injection into the foot may be suggested. This can be done as a day case without the need for anaesthesia and helps reduce inflation of the nerve. It can halt the pain in round 70 % of cases. Sometimes a combination of alcohol and local anaesthesia may be injected as this helps reduce pain.
Surgical Treatment
If symptoms do not respond to any of the above measures then surgery may be suggested. This involves a short 30 minute operation to either remove tissue to take pressure off the nerve or to remove the nerve causing the pain. The surgery can be done as a day case but it will be two or three weeks before you can be fully active on your feet. There may be some lingering numbness afterwards if the nerve is removed. But surgery is successful in around 80% of cases. There is a small risk of complications such as infection and thickening of the skin on the soles of the feet.
A neuroma develops when a nerve is compressed, injured or pinched, causing swelling and pain. A neuroma in the area between the third and fourth toes, or between the second and third toes, is known as a Morton?s neuroma. Morton?s neuroma causes sharp, burning pain and numbness in the toes and foot. You may feel like you?ve stepped on a tiny hot coal and can?t get rid of it. At the same time, you?ll have the disconcerting experience of not being able to feel your toes. Sometimes the nerve tissue becomes so thickened you can feel or see a lump.Causes
Various factors have been implicated in the precipitation of Morton's neuroma. Morton's neuroma is known to develop as a result of chronic nerve stress and irritation, particularly with excessive toe dorsiflexion. Poorly fitting and constricting shoes (ie, small toe box) or shoes with heel lifts often contribute to Morton's neuroma. Women who wear high-heeled shoes for a number of years or men who are required to wear constrictive shoe gear are at risk. A biomechanical theory of causation involves the mechanics of the foot and ankle. For instance, individuals with tight gastrocnemius-soleus muscles or who excessively pronate the foot may compensate by dorsiflexion of the metatarsals subsequently irritating of the interdigital nerve. Certain activities carry increased risk of excessive toe dorsiflexion, such as prolonged walking, running, squatting, and demi-pointe position in ballet.
Symptoms
Symptoms associated with a neuroma include a dull burning sensation radiating towards the toes, a cramping feeling, or even a stinging, tingling sensation that can be described as being similar to an electric shock. It is often worse when wearing shoes with most people finding the pain disappears when removing their shoes.
Diagnosis
To diagnose Morton's neuroma the podiatrist commonly palpates the area to elicit pain, squeezing the toes from the side. Next he or she may try to feel the neuroma by pressing a thumb into the third interspace. The podiatrist then tries to elicit Mulder's sign, by palpating the affected interspace with one hand and squeezing the entire foot at the same time with the other hand. In many cases of Morton's neuroma, this causes an audible click, known as Mulder's sign. An x-ray should be taken to ensure that there is not a fracture. X-rays also can be used to examine the joints and bone density, ruling out arthritis (particularly rheumatoid arthritis and osteoarthritis).
Non Surgical Treatment
The first line of treatment is to try modifying footwear. Often simply wearing broader fitting shoes can reduce pressure on the neuroma and so reduce pain. Orthotic inserts can also help as they can again help reduce pressure on certain parts of the foot. Padding and taping the toe area is another option. In some cases a steroid injection into the foot may be suggested. This can be done as a day case without the need for anaesthesia and helps reduce inflation of the nerve. It can halt the pain in round 70 % of cases. Sometimes a combination of alcohol and local anaesthesia may be injected as this helps reduce pain.
Surgical Treatment
If symptoms do not respond to any of the above measures then surgery may be suggested. This involves a short 30 minute operation to either remove tissue to take pressure off the nerve or to remove the nerve causing the pain. The surgery can be done as a day case but it will be two or three weeks before you can be fully active on your feet. There may be some lingering numbness afterwards if the nerve is removed. But surgery is successful in around 80% of cases. There is a small risk of complications such as infection and thickening of the skin on the soles of the feet.
Shoe Lifts For Leg Length Discrepancy
There are actually not one but two different types of leg length discrepancies, congenital and acquired. Congenital means you are born with it. One leg is structurally shorter compared to the other. As a result of developmental stages of aging, the brain picks up on the gait pattern and identifies some variation. The body usually adapts by tilting one shoulder over to the "short" side. A difference of under a quarter inch isn't grossly uncommon, does not need Shoe Lifts to compensate and generally won't have a serious effect over a lifetime.

Leg length inequality goes typically undiagnosed on a daily basis, however this problem is simply solved, and can reduce many incidents of back discomfort.
Treatment for leg length inequality typically consists of Shoe Lifts. Most are affordable, normally priced at under twenty dollars, compared to a custom orthotic of $200 plus. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Lumbar pain is the most prevalent ailment impacting men and women today. Over 80 million men and women experience back pain at some point in their life. It is a problem which costs companies millions of dollars every year on account of time lost and production. Fresh and improved treatment solutions are continually sought after in the hope of lowering economical impact this condition causes.

Men and women from all corners of the earth suffer from foot ache due to leg length discrepancy. In these types of cases Shoe Lifts can be of worthwhile. The lifts are capable of eliminating any discomfort and pain in the feet. Shoe Lifts are recommended by many experienced orthopaedic orthopedists.
To be able to support the human body in a healthy and balanced manner, the feet have a significant part to play. Inspite of that, it is sometimes the most overlooked zone in the human body. Many people have flat-feet meaning there is unequal force placed on the feet. This causes other body parts including knees, ankles and backs to be affected too. Shoe Lifts guarantee that correct posture and balance are restored.
Leg length inequality goes typically undiagnosed on a daily basis, however this problem is simply solved, and can reduce many incidents of back discomfort.
Treatment for leg length inequality typically consists of Shoe Lifts. Most are affordable, normally priced at under twenty dollars, compared to a custom orthotic of $200 plus. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Lumbar pain is the most prevalent ailment impacting men and women today. Over 80 million men and women experience back pain at some point in their life. It is a problem which costs companies millions of dollars every year on account of time lost and production. Fresh and improved treatment solutions are continually sought after in the hope of lowering economical impact this condition causes.
Men and women from all corners of the earth suffer from foot ache due to leg length discrepancy. In these types of cases Shoe Lifts can be of worthwhile. The lifts are capable of eliminating any discomfort and pain in the feet. Shoe Lifts are recommended by many experienced orthopaedic orthopedists.
To be able to support the human body in a healthy and balanced manner, the feet have a significant part to play. Inspite of that, it is sometimes the most overlooked zone in the human body. Many people have flat-feet meaning there is unequal force placed on the feet. This causes other body parts including knees, ankles and backs to be affected too. Shoe Lifts guarantee that correct posture and balance are restored.
Just What Is Inferior Calcaneal Spur

Overview
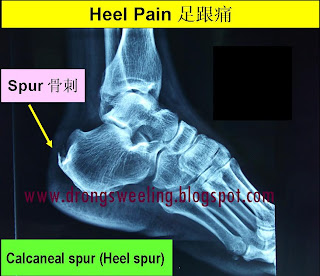
Heel spurs are a relatively common cause of heel pain. A heel spur is a pointed bone fragment that extends forward from the bottom of the heel from the heel bone, also referred to as a calcaneous. Serious pain and discomfort often develops with this condition. In many cases, a heel spur develops along with plantar fasciitis which occurs when the plantar fascia ligament becomes inflamed.
Causes
Heel spurs form in some patients who have plantar fasciitis (PLAN-tar fash-ee-I-tis), and tend to occur in patients who have had the problem for a prolonged period of time. While about 70 percent of patients with plantar fasciitis have a heel spur, X-rays also show about 50 percent of patients with no symptoms of plantar fasciitis also have a heel spur.
Symptoms
More often than not, heel spurs have no signs or symptoms, and you don?t feel any pain. This is because heel spurs aren?t pointy or sharp pieces of bone, contrary to common belief. Heel spurs don?t cut tissue every time movement occurs; they?re actually deposits of calcium on bone set in place by the body?s normal bone-forming mechanisms. This means they?re smooth and flat, just like all other bones. Because there?s already tissue present at the site of a heel spur, sometimes that area and the surrounding tissue get inflamed, leading to a number of symptoms, such as chronic heel pain that occurs when jogging or walking.
Diagnosis
A Diagnosis of Heel Spur Syndrome is a very common reason for having heel pain. Heel pain may be due to other types of conditions such as tendonitis, Haglund's Deformity, Stress Fracture, Tarsal Tunnel Syndrome, or low back problems. A more common condition in children is Sever's Disease. The diagnosis is usually made with a combination of x-ray examination and symptoms.
Non Surgical Treatment
The majority of heel spurs are treated with non-surgical interventions. These can relieve pain, but may take from about 3 months to up to a year for symptoms to resolve. Rest, icing, and over-the-counter anti-inflammatory or prescription medications can help ease symptoms. Cortisone injections may also be used. Physical therapists may instruct you to perform stretching exercises to help relax the tissues in the heel. Your doctor may recommend custom orthotics or shoe inserts to position and cushion your heel. Night splints can help position the heel and arch of the foot while you sleep. Some doctors may recommend extracorporeal shock wave therapy (ESWT). This treatment uses energy pulses to start the repair process in the heel tissues. ESWT is recommend when other non-surgical treatments have failed.
Surgical Treatment
Most studies indicate that 95% of those afflicted with heel spurs are able to relieve their heel pain with nonsurgical treatments. If you are one of the few people whose symptoms don?t improve with other treatments, your doctor may recommend plantar fascia release surgery. Plantar fascia release involves cutting part of the plantar fascia ligament in order to release the tension and relieve the inflammation of the ligament. Sometimes the bone spur is also removed, if there is a large spur (remember that the bone spur is rarely a cause of pain. Overall, the success rate of surgical release is 70 to 90 percent in patients with heel spurs. One should always be sure to understand all the risks associated with any surgery they are considering.
What Causes Heel Spur
Overview
Patients and doctors often confuse the terms heel spur and plantar fasciitis. While these two diagnoses are related, they are not the same. Plantar fasciitis refers to the inflammation of the plantar fascia--the tissue that forms the arch of the foot. A heel spur is a hook of bone that can form on the heel bone (calcaneus) and is associated with plantar fasciitis. About 70 percent of patients with plantar fasciitis have a heel spur that can be seen on an X-ray. However, many patients without symptoms of pain can have a heel spur. The exact relationship between plantar fasciitis and heel spurs is not entirely understood.
Causes
A strong band of sinew (plantar fascia) stretches across the sole of the foot below the surface of the skin and is attached to a point in the middle of the under surface of the heel bone. With repeated activity on our feet, the plantar fascia can become tight and cause persistent traction (tugging) on its attachment point into the heel bone, and inflammation and pain may develop at this site. This painful condition is known as plantar fasciitis. Sometimes a ?spur? develops at the site of this traction on the bone and protrudes into the surrounding tissue. This is a heel spur.

Symptoms
Heel spurs are most noticeable in the morning when stepping out of bed. It can be described as sharp isolated pain directly below the heel. If left untreated heel spurs can grow and become problematic long-term.
Diagnosis
Your doctor, when diagnosing and treating this condition will need an x-ray and sometimes a gait analysis to ascertain the exact cause of this condition. If you have pain in the bottom of your foot and you do not have diabetes or a vascular problem, some of the over-the-counter anti-inflammatory products such as Advil or Ibuprofin are helpful in eradicating the pain. Pain creams, such as Neuro-eze, BioFreeze & Boswella Cream can help to relieve pain and help increase circulation.
Non Surgical Treatment
In case of heel spurs rest is most important. Active sports, running, long walks etc should be avoided to start with. If you?re in a job that requires a lot of standing, take a few days off work. Rest (or reduced activity) is essential to allow the inflammation from becoming aggrevated. Furthermore, you can use ice packs (placed on the heel for 5-10 minutes) to ?cool down? the inflamed area. You may take anti-inflammatory medication or apply a topical inflammatory (i.e. a cream) to help reduce inflammation. In addition, there are some simple exercises that should be done daily to help relieve heel spur pain.
Surgical Treatment
When chronic heel pain fails to respond to conservative treatment, surgical treatment may be necessary. Heel surgery can provide relief of pain and restore mobility. The type of procedure used is based on examination and usually consists of releasing the excessive tightness of the plantar fascia, called a plantar fascia release. Depending on the presence of excess bony build up, the procedure may or may not include removal of heel spurs. Similar to other surgical interventions, there are various modifications and surgical enhancements regarding surgery of the heel.
Prevention
Use orthotic inserts. You can purchase orthotics over the counter, or you can have orthotics specially fitted by your podiatrist. Try 1 of these options. Heel cups. These inserts will help to align the bones in your foot and to cushion your heel. Check your skin for blisters when you first start using heel cups. Also, your feet may sweat more with a heel cup, so change your socks and shoes often. Insoles. While you can pick up generic insoles at a drugstore, you may have more luck if you go to a store that sells athletic shoes. Push on the arch to make sure that it doesn't collapse. If your insoles help but could use a little work, you can take them to a podiatrist to get them customized. Custom orthotics. A podiatrist can make a cast of your foot and provide you with custom-made orthotics. These may be more expensive, but they are made of materials specifically designed for your needs, and they can last up to 5 years if your podiatrist refurbishes them every 1 or 2 years. To find a podiatrist near you, look at the Web page for the American Academy of Podiatric Sports Medicine. Dynamic Insoles. Lack of elasticity in plantar fascia in the foot is for most people the real problem. If there is poor elasticity in the lengthwise tendons in the foot (plantar fascia) in relation to a person's general condition, only a small additional strain is required for the pull on the tendons to cause damage to the tissues connecting the tendons to the heel bone. This will generate an inflamed condition called Plantar Fasciitis.